|
CONGENITAL
HYPOTHYROIDISM |
Fetal hypothalamic-pituitary-thyroid axis is intact and functional by 12 weeks of gestation.
Abnormal thyroid function in the fetus poses three main risks:
- Cretinism and mental retardation due to hypothyroidism.
- Airway obstruction from an enlarged thyroid.
- Polyhydramnios probably due to mechanical esophageal obstruction. Fetal inspiration and swallowing are important in amniotic fluid circulation.
ETIOLOGY |
- 80% due to thyroid gland dysgenesis.
- 10-20% due to thyroid hormone dysgenesis
- <5% due to a hypothalamic pituitary disorder.
Note: The fetus converts T4 to T3 and especially
reverse T3 (a relatively inactive storage form of thyroid hormone not
present in the adult). Thyroxine does not cross the
placenta but antithyroid agents eg.
prophylthiouracil (PTU) does
cross freely from mother to fetus.
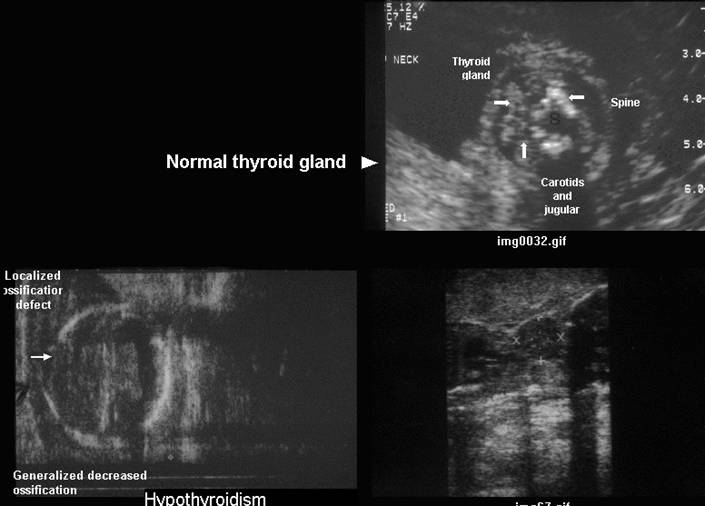
ULTRASOUND |
- Anterior neck mass from an enlarged goitrous gland. Occasionally it may be small and hypoplastic.
- Delayed bone age.
- Polyhydramnios.
- Skull - generalized deossification or focal ossification defects.
REFERENCES |
- Weiner S, Scharf JI, Bolognese RJ, Librizzi RJ. Antenatal Diagnosis and treatment of a Fetal Goiter. The Journal of Reproductive Medicine 1980, 24:39-42.
- Perelman AH, Johnson RL,