|
ULTRASOUND OF
COMPLETE MOLAR PREGNANCY IN THE
FIRST TRIMESTER |
·
It si
now recognized that the majority of partial and complete moles present both
clinically and sonographically as early pregnancy
failure.
·
Most first trimester pregnancies affected by hydatidiform mole are evacuated prior to the development of
the classic features described in the second trimester. Both sonographic (1,2) and pathological findings may be quite different in cases from
hydatidiform moles presenting and evacuated in early
gestations (3). Early ultrasound-based literature
reported that HM could be easily recognized in the second trimester, being
associated with numerous vesicular structures filling the uterine cavity, often
with a  snowstorm
snowstorm appearance, with or without coexistent ovarian theca-lutein
cysts. It is now clear that such features are rarely present in the first
trimester,
appearance, with or without coexistent ovarian theca-lutein
cysts. It is now clear that such features are rarely present in the first
trimester,
·
In a recent paper by Sebire et.al. (4), a
sonographic diagnosis of missed abortion or anembryonic pregnancy with no
documented sonographic suspicion of molar pregnancy was identified in 67% of
cases. This highlights the importance of complete histopathological
analysis of the products of conception to exclude gestational trophoblastic disease.
·
At this early gestation, however,
marked hydropic change may be absent, both pathologically and on ultrasonographic
or naked eye examination, the products initially appearing indistinguishable
from non-molar miscarriage at the time of evacuation.
·
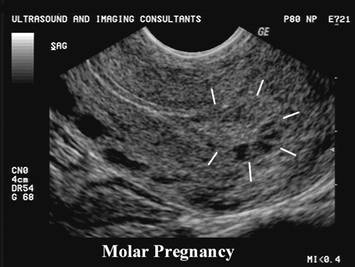
In the absence of an embryo/fetus, the finding of
apparent molar change on first-trimester ultrasound examination is most likely
to represent true molar change, usually complete hydatidiform
mole, but histological confirmation is still required since occasional hydropic abortions may have a similar appearance and the
distinction between partial and complete mole can only be made histologically/cytogenetically.
·
The majority of cases are
therefore now detected following routine histopathological
examination of products of conception.
|
|
|
|
|
|



·
In the presence of an embryo/fetus at any gestation,
there are three possibilities:
o The
pregnancy is an androgenetic triploidy
(partial mole) with significant embryonic development.
o The pregnancy
may be a twin pregnancy with a complete mole and a normal twin.
o Other
specific pathological conditions may be present which mimic hydatidiform
moles, such as the mesenchymal dysplasia/stem
vessel hydrops spectrum (5).
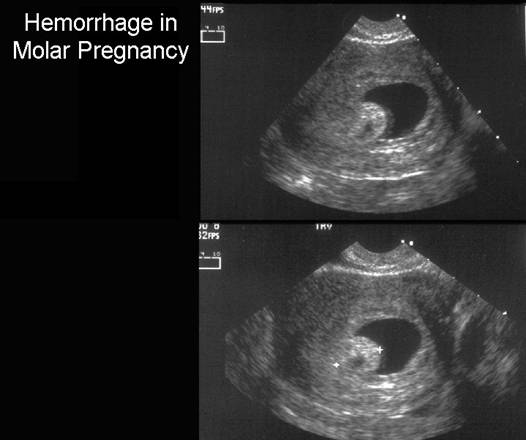
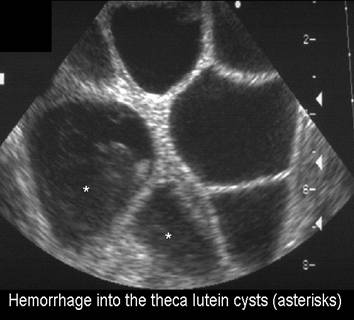
- Hemorrhage is rare, but sonographically presents as an echogenic nodule (7).
|
ULTRASOUND OF
COMPLETE MOLAR PREGNANCY IN THE
SECOND TRIMESTER |
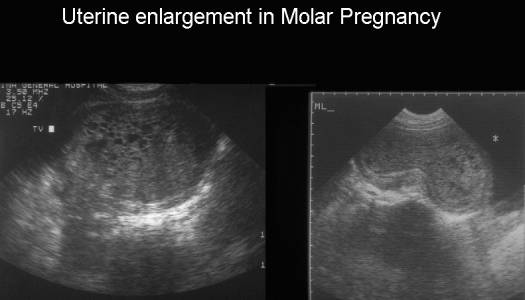
- Uterine signs.
- Uterine enlargement (60%)
|
|
|
|
|
|
Video clip of echogenic
(hemorrhagic) Molar Pregnancy
|
|
|
|
|
|

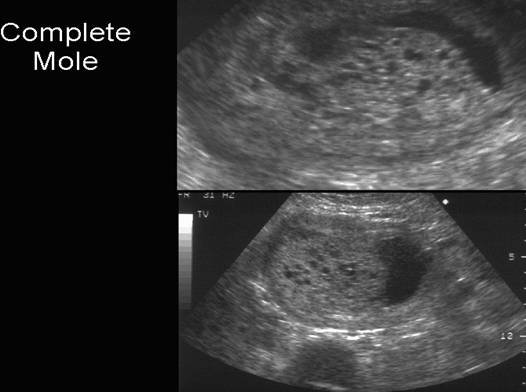
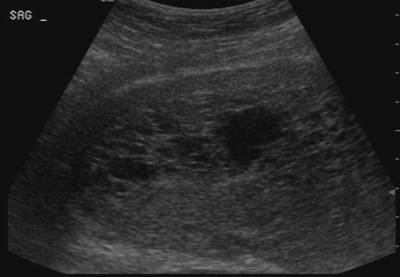
- Echogenic central uterine mass.
- Numerous discrete anechoic (cystic) spaces + central area of heterogeneous echotexture ("snowstorm appearance"). Cystic areas are hydropic villi. This classical appearance is only present in less than two-thirds of cases and is less common in the first trimester (2). The vesicles may be too small and the interfaces too numerous to distinguish as cystic spaces.
|
|
|


- Size of the villi is directly proportional to gestational age (6); early molar pregnancies may therefore not demonstrate the typical sonographic pattern described above.
- Occasionally may present as a large, central filled collection that looks like an anembryonic gestation, missed or incomplete abortion.
- Other atypical appearances include a cluster of hypoechoic structures surrounded by an echogenic rim (8).
- Ovarian signs.
- Ovarian enlargement
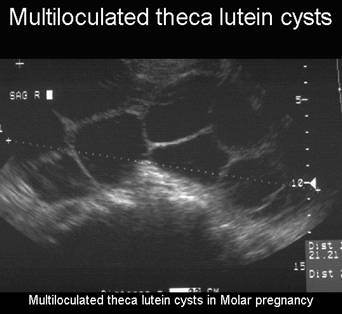
- Theca lutein cysts - up to 40% of cases (probably an overestimation). Arises due to hyper stimulation resulting from the high circulating levels of bhCG. These levels often do not rise until early in the second trimester and therefore theca lutean cysts are rare in early molar pregnancies (9).
- Theca lutein cysts are:
- Multiloculated.
- Usually bilateral.
- Resolve after treatment.
- Hemorrhage or rupture rare.
|
|
|
- Also caused by twin gestations, fetal hydrops, stimulation with human maternal gonadotropin and occasionally a normal pregnancy.
- Some authors believe that the presence of theca lutein cysts should alert one to an increased probability of one of the more aggressive forms of GTD (invasive mole or choriocarcinoma) (9,10).
- Fetus.
- No associated embryonic or fetal structures.
- May co-exist with a normal fetus and placenta in cases of molar transformation of one ovum in a dizygotic twin pregnancy.
- Twin pregnancies that include complete hydatidiform mole and coexistent fetus have a greater malignant potential and must be distinguished from partial molar pregnancy (and a triploid fetus).
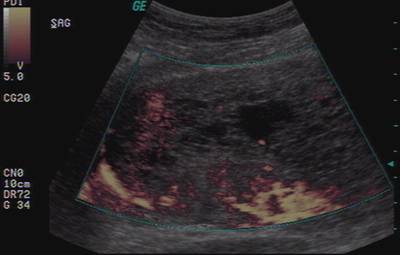
- Doppler studies.
- There is a low uterine arterial resistance to flow with high peak systolic velocities (6).
- Doppler US may be useful in the evaluation of GTD. These vascular tumors tend to show very high blood flow. More specifically, high diastolic flow, presumably the result of decreased vessel tone in the proliferating neoplasm, has been identified in patients with persistent gestational trophoblastic neoplasia (16-18). Although this decrease in uterine artery pulsatility may be of some use in diagnosing confusing cases that occasionally clinically mimic other conditions (eg, threatened abortion or uterine atony) (19,20), the persistently elevated beta-hCG level will usually indicate the diagnosis (21,22).
- Fine et al. (11) examined 22 cases of partial mole and compared the sonographic features with those of non-molar abortions and reported that cystic changes and increased echogenicity in the placenta may be useful features to predict molar pregnancy.
- Lazarus et al. (12) examined 21 cases of complete hydatidiform mole at 4–18 weeks of gestation and reported that the diagnosis of molar pregnancy was made in 57% of the cases and in no cases were theca lutein cysts present.
- More recently, Benson et al. (13) described 24 cases of complete molar pregnancies examined sonographically in a specialist center and reported that molar pregnancy was suspected on ultrasound examination in 79% of cases, suggesting, as with all sonographic techniques, that experienced operators may achieve a higher rate of diagnostic accuracy.
- Jauniaux et al. (14) reported that 10 of 11 cases of pregnancies with sonographic molar placental change identified at 10–14 weeks of gestation were pathologically proven complete or partial moles, in keeping with our finding of a relatively high positive predictive value of a sonogram, which suggests molar change.
- Lindholm et al. (15) reported that on the basis of sonography and macroscopic examination of products of conception for molar change, approximately 80% of complete moles and 30% of partial moles could be detected, but in several cases macroscopic examination at the time of uterine evacuation raised the first clue to the diagnosis, further demonstrating the need for routine histopathological assessment in all such cases.
- MRI studies - The use of MR imaging for
evaluating these lesions has been described (25). In general, the lesions
are heterogeneous, hypervascular masses that
distort the normal zonal anatomy. Abnormal signal intensity may be seen in
the myometrium or parametrium.
The authors of one large series noted a return to a normal appearance
after therapy and clinical resolution of the disease (26). The impact of
MR imaging findings on management decisions was minimal (26). Therefore,
rather than be a standard part of the evaluation, MR imaging is more
likely to serve as a problem-solving tool in selected cases (25,26).
- The single largest
previous study reporting specifically on the diagnostic accuracy of
routine ultrasound examination in non-specialist centers for the detection
of histologically confirmed molar pregnancy was
from a Regional Trophoblastic Disease
Surveillance Centre (27). In this study, of almost 200 consecutive
pregnancies referred with a diagnosis of possible HM, there were 155 cases
with a final review diagnosis of complete or partial mole. In 131 (67%) of
these cases, the pre-evacuation sonographic diagnosis was that of a simple
missed abortion/anembryonic pregnancy with no
documented suspicion of molar change, referral being on the basis of
findings at routine histological examination of products of conception. In
63 pregnancies ultrasound examination suggested HM, and in 53 (84%) of
these the diagnosis of molar pregnancy was correct, demonstrating
relatively high specificity for the ultrasound findings but also
highlighting that non-molar hydropic miscarriage
may occasionally mimic HM sonographically.
Overall, 37/64 (58%) complete moles and 16/91 (17%) partial moles had a
correct pre-evacuation diagnosis of GTN; in total, only 53/155 (34%) HM
cases were suspected as being molar on sonographic examination.
DIFFERENTIAL DIAGNOSIS |
- Uterine dysgerminoma.
- Uterine sarcoma.
- Uterine lymphangioma.
Unlike complete molar pregnancy, the bhCG and a-fetoprotein levels are normal in 1, 2 and 3 above.
- Non molar miscarriage (missed abortion) (27).
|
|
|
|
|
|

REFERENCES |
- Woodward RM, Filly RA, Callen PW. First trimester molar pregnancy: nonspecific ultrasonographic appearance. Obstet Gynecol 1980; 55: 31S–33S
- Lazarus E, Hulka C, Siewert B, Levine D. Sonographic appearance of early complete molar pregnancies. J Ultrasound Med 1999; 18: 589–94
- Paradinas FJ. The histological diagnosis of hydatidiform moles. Curr Diagnostic Pathol 1994; 1: 24–31
- Jauniaux E, Nicolaides KH, Hustin J. Perinatal features associated with placental mesenchymal dysplasia. Placenta 1997; 18: 701–6
- Szulman AE, Surti U. Linear relationship between gestational age and size of villi. Am J Obstet Gynecol 1978;132:20.
- Bronson RA, van de Gegte GL. An unusual first-trimester sonographic finding associated with development of hydatidiform mole. AJR 1992;160:137.
- Crade M, Weber PR. Appearance of molar pregnancy 9.5 weeks after conception. J Ultrasound Med 1991;10:473.
- Wagner BJ, Woodward PJ, Dickey GE. Gestational trophoblastic disease: Radiologic - Pathologic correlation. Radiographics 1996;16:131-148.
- Jauniaux E. Ultrasound diagnosis and follow-up of gestational trophoblastic disease. Ultrasound Obstet Gynecol 1998;11:367-377.
- Fine C, Bundy AL, Berkowitz RS et.al. Sonographic diagnosis of partial hydatidiform mole. Obstet Gynecol 1989; 73: 414–8
- Lazarus E, Hulka C, Siewert B, Levine D. Sonographic appearance of early complete molar pregnancies. J Ultrasound Med 1999; 18: 589–94
- Benson CB, Genest DR, Bernstein MR et.al. Sonographic appearance of first trimester complete hydatidiform moles. Ultrasound Obstet Gynecol 2000; 16: 188–91
- Jauniaux E, Nicolaides KH. Early ultrasound diagnosis and follow-up of molar pregnancies. Ultrasound Obstet Gynecol 1997; 9: 17–21
- Lindholm H, Flam F. The diagnosis of molar pregnancy by sonography and gross morphology. Acta Obstet Gynecol Scand 1999; 78: 6–9
- Caspi B, Elchalal U, Dgani R, Ben-Hur H, Rozenman D, Nissim F. Invasive mole and placental site trophoblastic tumor: two entities of gestational trophoblastic disease with a common ultrasonographic appearance. J Ultrasound Med 1991; 10:517-519.
- Mangili G, Spagnola D, Valsecchi L, Maggi R. Transvaginal ultrasonography in persistent trophoblastic tumor. Am J Obstet Gynecol 1993; 169:1218-1223.
- Schneider DF, Bukovsky I, Weinraub Z, Golan A, Caspi E. Transvaginal ultrasound diagnosis and treatment follow-up of invasive gestational trophoblastic disease. J Clin Ultrasound 1990; 18:110-113.
- Desai RK, Desberg AL Diagnosis of gestational trophoblastic disease: value of endovaginal color flow Doppler sonography. AJR 1991; 157:787-788.
- Carter J, Fowler J, Carlson J, et al. Transvaginal color flow Doppler sonography in the assessment of gestational trophoblastic disease. J Ultrasound Med 1993; 12:595-599
- Kurjak A, Zalud I, Predanic M, Kupesic S. Transvaginal color and pulsed Doppler study of uterine blood flow in the first and second trimesters of pregnancy: normal versus abnormal. J Ultrasound Med 1994; 13:43-47.
- Achiron R, Goldenberg M, Lipitz S, Mashiach S. Transvaginal duplex Doppler ultrasonography in bleeding patients suspected of having residual trophoblastic tissue. Obstet Gynecol 1993; 81:507-511.
- Kohorn EI. Evaluation of the criteria used to make the diagnosis of nonmetastatic gestational trophoblastic neoplasia. Gynecol Oncol 1993; 48:139-147.
- Schlaerth JB. Nonmetastatic gestational trophoblastic neoplasms (editorial). Gynecol Oncol 1993; 48:137.
- Hricak
H, Demas BE,
- Sebire NJ,
Rees H, Paradinas F, Seckl
M, Newlands E. The diagnostic implications of
routine ultrasound examination in histologically
confirmed early molar pregnancies. Ultrasound
Obstet Gynecol
2001; 18: 662-665.