|
ULTRASOUND OF ECHOGENIC BOWEL GRADING SYSTEM FOR ECHOGENIC BOWEL (1) |
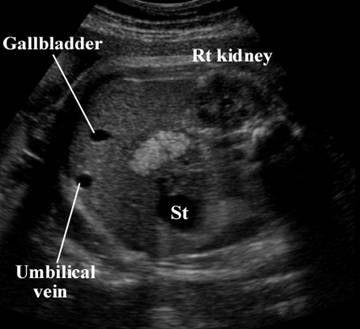
· Fetal echogenic bowel refers to the presence of hyperechoic, or bright bowel, as compared with the echogenicity of adjacent bone diagnosed in the second trimester of pregnancy. Echogenic bowel in the third trimester is a relatively common finding with uncertain clinical significance.
· This finding can be diffuse or focal.
· This is done by turning down the gain setting until other soft tissues are no longer seen and only bone or bowel is visible.
· There is significant interobserver and intraobserver variation
Grade
|
Sonographic appearance
|
Frequency of associated abnormalities
|
0
|
Normal bowel echogenicity
|
0%
|
|
|
|
|
1
|
Echogenicity increased but
less than the iliac crest
|
0%
|
|
|
|
|
|
|
|
|
2
|
Echogenicity similar to
that of the iliac crest
|
5%
|
|
|
|
|
|
|
|
|
3
|
Echogenicity greater than that
of the iliac crest.
|
46%
|
|
|
|
|
|
|
|
|





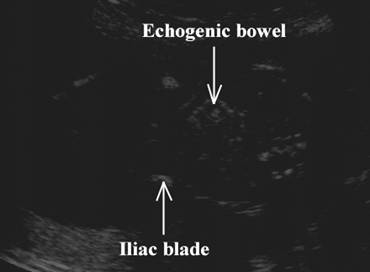

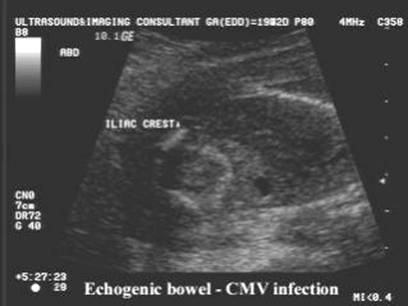
- Iliac crest is used as an internal standard as it can usually be imaged at the same level as the bowel.
- Increasing echogenicity (and therefore a higher grade) correlates with increased risk of a fetal abnormality.
- Despite these limitations, the association of echogenic bowel with adverse pregnancy outcomes is strongest with moderate-to-severe echogenicity, when the bowel is as echogenic as or more echogenic than bone.
|
CMV infection |
|
|
|
|
|
|
|
|
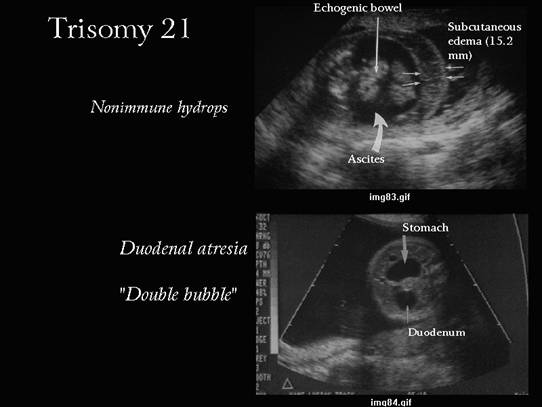
Trisomy
21 |
|
|
|
|



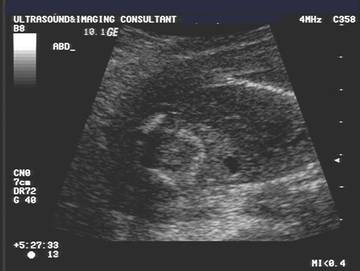
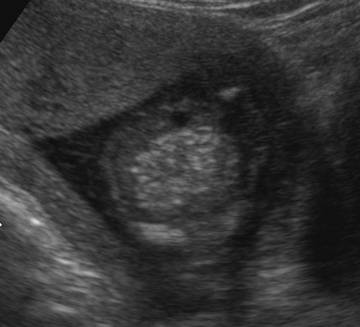
- Bowel must be investigated with a 3.5 or 5.0Mhz transducer as some workers (2,3) have observed hyperechogenic bowel in normal fetuses when scanned with 6.5 or 8Mhz transducers.
|
|
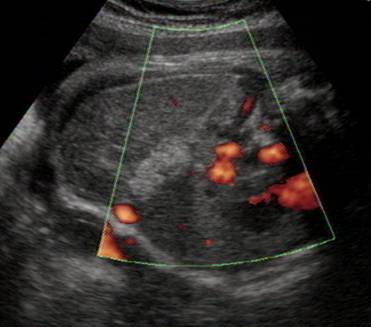
Echogenic bowel – 7.5 MHz transducer |

The finding of true echogenic bowel at the time of second-trimester ultrasound should prompt a work-up that targets these findings.
· A detailed ultrasound of the fetus should be performed (careful evaluation of the amniotic fluid, placenta, and membranes for any features of intra-amniotic bleeding, such as particulate debris or clot floating in the amniotic fluid or chorioamniotic separation).
· An amniocentesis for karyotype probably should be recommended even when echogenic bowel is an isolated finding.
· CF carrier testing for both parents should be recommended.
· Maternal serologic testing for evidence of recent CMV and toxoplasmosis should be performed (IgG and IgM). If there is evidence of recent infection, an amniocentesis can be performed and the amniotic fluid tested for evidence of CMV, toxoplasmosis, and parvovirus infection.
· Because these fetuses are at risk for IUGR, these fetuses should be followed with serial growth scans.
REFERENCES
|
- Slotnick R, Abuhamad A. Prognostic implications of fetal echogenic bowel. Lancet 1996;347:85-87.
- Perez CG, Goldstein RB. Sonographic borderlands in the fetal abdomen. Seminars in Ultrasound, CT, and MRI 1998;19(4):336-346.