|
NORMAL VARIANTS AND
PITFALLS |
- Echogenic intracardiac focus
- Pseudo-ventricular septal defect when the ultrasound beam is parallel to the membranous portion of the septum (it is probably due to the thin membranous septum). Scan interventricular septum with the ultrasound beam perpendicular to the septum to correct this pitfall.
- Redundant flap of foramen ovale.
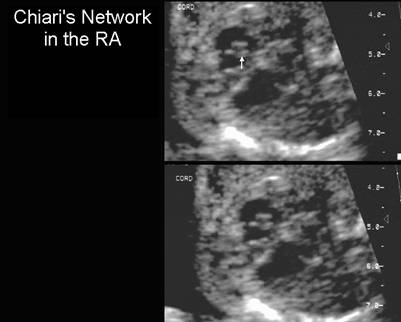
May appear circular and mimic an aneurysm of the atrial septum or the aortic root. - Chiari's
network in the right atrium.
Thin filamentous mobile echoes in the right atrium results when the resorptive process of the embryonic right valve of the sinus venosus leaves a fenestrated or reticular network of fibers.
|
|
- Pericardial fluid - Fluid measuring £ 2mm is a normal finding.
- Hypoechoic
dropout from the myocardium.
The peripheral hypoechoic portion of the myocardium may lead to an overdiagnosis of pericardial effusion. The rim measures 0.6 - 6mm and can be seen in over 94% of fetal hearts. This pitfall probably arises from the difference in orientation of the muscle fibres in the ventricle. The longitudinal fibres are located closer to the ventricular lumen, while the circular fibers, located peripherally, are the likely cause for this appearance. - Echogenic
focus at the edge of the myocardium.
A brightly echogenic focus at the edge of the ventricular myocardium is not a tumor or area of myocardial calcification. It represents the anterior edge of a rib or part of the sternum.


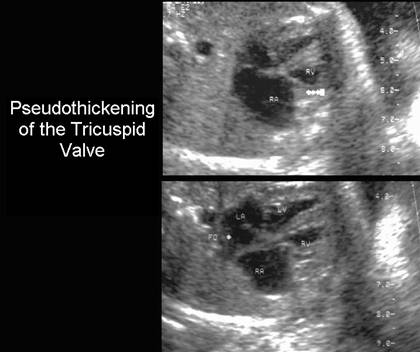
- Pseudothickening
of the Tricuspid Valve
A parietal band (the supraventricular crest) is an arch shaped band of muscle located between the tricuspid and pulmonary valves. This can be mistaken for a thickened tricuspid valve.
|
|
- Entrance
of coronary sinus into the right atrium
The coronary sinus returns venous blood from the myocardium to the right atrium. It opens into the right atrium between the tricuspid valve and the entrance of the IVC. In some imaging planes the entrance of the coronary sinus into the right atrium may simulate a defect in the lower atrial septum. - Pseudo-overriding of the
aorta
On the long-axis view of the left ventricular outflow tract, continuity of the ventricular septum with the anterior wall of the aorta is important to demonstrate. Overriding aorta is found in tetralogy of Fallot. Pseudo-overriding is thought to be due to a combination of thinness of the membranous septum, the normal left ventricular outflow tract and partial volume artifact with the pulmonary outflow tract or with a sinus of Valsalva. One needs to obtain the long axis view in a slightly different plane. - Parallel course of the
outflow tracts distal to the semilunar valves
Parallel course proximal to the semilunar valves is abnormal and suggests transposition, however distal to the valves at the level of the aortic arch, the aorta and pulmonary artery-ductus arteriosus do run parallel for a short distance. - Normal dilatation of the
pulmonary artery.
The pulmonary artery caliber increase slightly just distal to the pulmonary valve (where it trifurcates into the ductus arteriosus and left and right pulmonary arteries). This should not be mistaken for poststenotic dilatation (associated with pulmonary stenosis).
REFERENCES |
- Brown DL, DiSalvo DN, Frates MC et.al. Sonography of the fetal heart: normal variants and pitfalls. AJR 1993;160:1251-1255.