|
· Patients given a
choice whether or not she wishes to be screened (patients ³ 35yrs offered
amniocentesis).
· Counseling about the test and it's implications
should precede screening.
· Need safeguards to deal with patient anxiety.
|
Detection rate
|
False +ve
|
Odds of being affected if +ve
|
|
MA>35yrs
31%
MA+aFP
33%
MAA+MSS
60%
|
7.5%
5%
5%
|
1:150
1:89
1:35
|
MA (Maternal age)
· Rationale for selecting 35, was the risk of
chromosomal abnormality versus risk of procedural miscarriage = 1:200
Problem: 60-80 Down Syndrome occur in pregnancies < 35 years
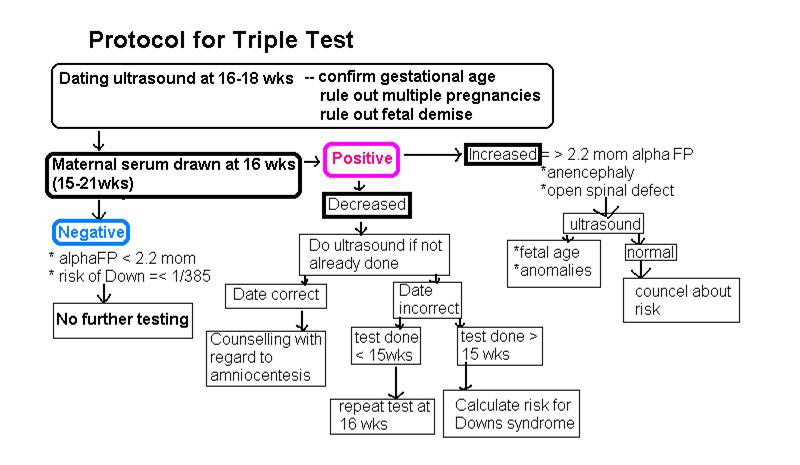
aFP
· Increased in neural tube defects
· Decreased 25% in Down Syndrome
MSS
· hCG in maternal serum=2x higher in Down
· uE3 in maternal serum=25% lower in Down
· hCG, uE3 Decreased in Trisomy 18
|
1. Maternal weight (heavy females have a lower aFP).
hCG and uE3 are also affected by maternal weight.
2. Insulin dependent diabetes
aFP ± 20% lower. Adjustment divided
by 0.8.
hCG and uE3 less affected.
3. Race - Black 10-15%.
4. Smoking - hCG 20-30% lower in smokers.
5. Gestational Age.
All 3 measurements depend on GA.
Need Ultrasound to:
· Establish
GA.
· Confirm singleton pregnancy.
· Exclude abnormality eg anencephaly.
· Reduce false positive rate and therefore patients
anxious by the test.
Therefore dating ultrasound prior to screening enhances the effectiveness of
screening.
|