|
SULCI AND GYRI |
Sonographic appearance of the sulci and gyri depend on the higher echogenicity of the pia-mater and pia-arachnoid complex (leptomeninx).
Sulcus = indentation at the expected location of the initially smooth cortical surface.
Insula assessed by evaluating the age at which opercular overfolding changed from obtuse to acute.
|
ULTRASOUND |
- Early in the second trimester the normal brain is still quite smooth and abnormal cortical development should not be diagnosed before 20 weeks of gestation.
- Left-right symmetry of time of appearance of sulci is the rule in anatomical studies (1-4) but a few exceptions are reported.
o Dorovini-Zis and Dolman evaluated symmetry in 23/80 brain samples and reported that 5/23 showed left-right differences (2). In three cases the right superior temporal sulcus was evident earlier. In two cases the central sulcus appeared earlier, once on the right and once on the left.
o Chi et al. reported that the right superior frontal and superior temporal sulci, secondary sulci and right insular sulci were visible 1-2 weeks earlier than the left (1).
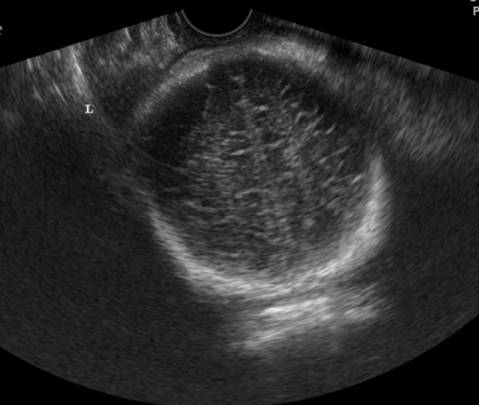
- Sulci are easier to detect enface in a direction perpendicular to their plane of orientation.
o Sulci on the hemisphere farther from the transducer are seen more clearly than those in the near field.
o Sulci on the medial surfaces of the hemispheres, specifically the parieto-occipital fissure, calcarine sulcus and cingulate sulcus, appeared earlier and are more confidently seen than convexity sulci.
o The
earliest appearance of a sulcus was as a small ![]() dot
dot![]() in
the expected site of the sulcus.
in
the expected site of the sulcus.
o Later,
the sulci formed an obvious ![]() V
V![]() indentation.
indentation.
o Finally,
the sulci became deeper and were visible as a surface
notch and an echogenic line extending into the brain matter in a ![]() Y
Y![]() configuration
configuration
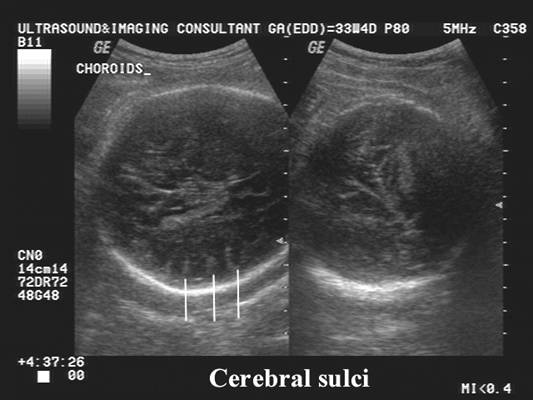
- When imaged in a direction parallel to their plane of orientation, sulci appear as an echogenic plate that should not be mistaken for a disorder of the brain parenchyma. This is especially true of the calcarine sulcus, which on axial views can be seen as an echogenic band on the medial surface of the occipital lobe just medial to the occipital horn.
- Anatomical reports of sulcal appearance times differ by as much as 4-6 weeks (1,2).
- Generally, sulcal detection by imaging studies lags behind their anatomical appearance.
o The identification of the parieto-occipital fissure and calcarine sulcus by imaging lags behind anatomical identification by about 2 weeks (anatomy 16 weeks vs. ultrasound and MRI 18 weeks).
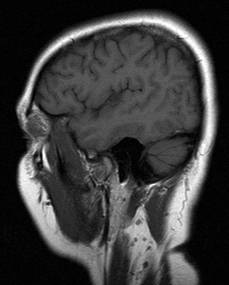
o The cingulate sulcus is more difficult to see and its appearance on ultrasound and MRI lags anatomical descriptions by about 7 weeks (anatomy 16 weeks vs. ultrasound 23 weeks and MRI 24 weeks).
|
Sulcus |
Threshold (first seen) (wks) |
Sulcus always
seen (wks) |
|||||||||||||
|
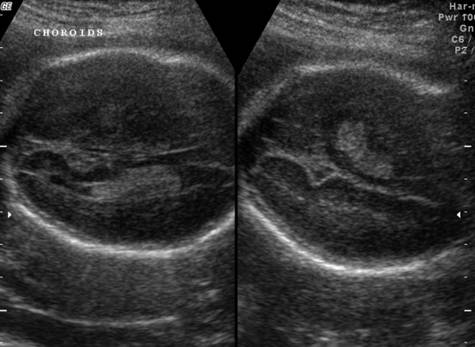
Parieto – occipital |
18.5 |
20.5 |
|||||||||||||
|
Best imaged axially
in a plane near the upper margin of the occipital horns of the lateral
ventricles. It first appeared
at 18.5 weeks, and was always visible after 20.5 weeks. |
|||||||||||||||
|
|
|
||||||||||||||
|
|
|
||||||||||||||
|
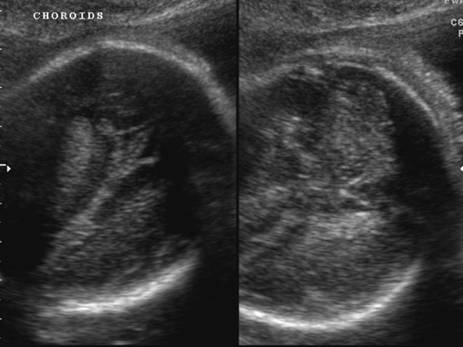
Calcarine |
18.5 |
21.9 |
|||||||||||||
|
Best imaged in a
coronal plane through the occipital lobes. It could be seen as
early as 18.5 weeks and was always visible after 21.9 weeks. |
|||||||||||||||
|
|
|
||||||||||||||
|
|
|
||||||||||||||
|
|
|
||||||||||||||
|
|
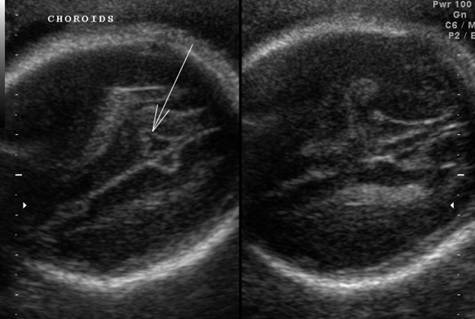
23.2 |
24.9 |
|||||||||||||
|
·
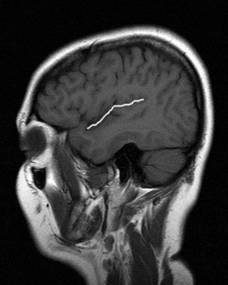
The cingulate sulcus was generally
not as confidently seen. It was best imaged in a coronal plane above the
region of the thalami. It became visible by 23.2 weeks in some fetuses and
was always seen after 24.3 weeks |
|||||||||||||||
|
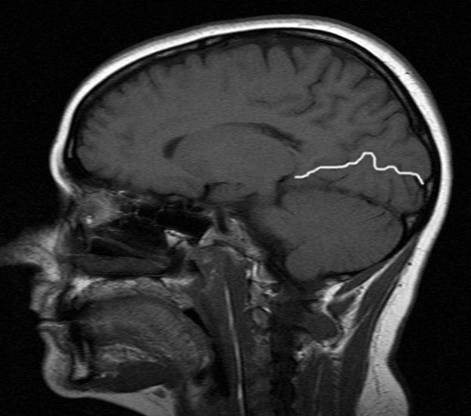
White = cingulated sulcus Red = parieto-occiptal sulcus |
|
||||||||||||||
|
Insula / Sylvian |
First acute |
Always acute |
|||||||||||||
|
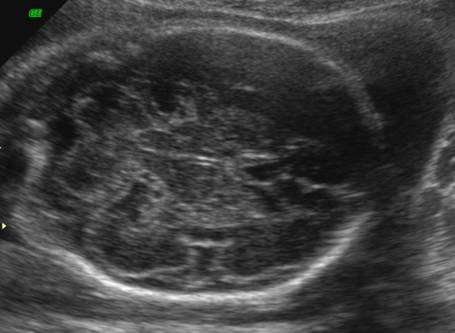
Insula – axial view |
23.5 |
24.4 |
|||||||||||||
|
Insula – coronal view |
23.2 |
24.9 |
|||||||||||||
|
|
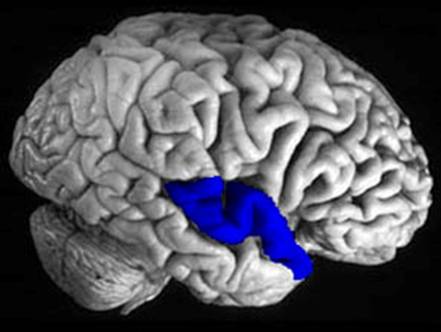
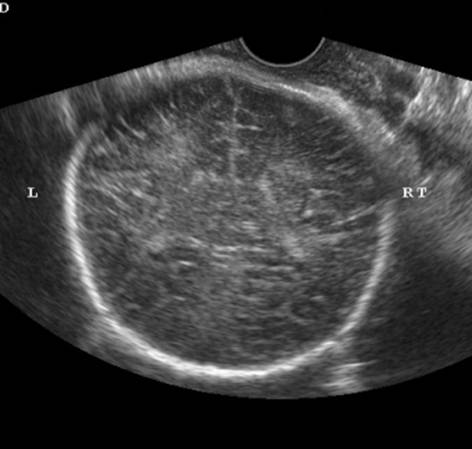
-
Has a
characteristic pattern of development. o
In
early pregnancy the Sylvian fossa is a smoothly
margined indentation. o
By
18-22 weeks' gestation the smooth Sylvian fossa
indentation developed angular margins at the site of the developing circular sulcus. This resulted in a plateau-like appearance with
angularity at the margins (the circular sulcus)
where the insula meets the frontal, parietal and
temporal opercula anteriorly, superiorly and posteriorly. These angles were initially obtuse but
became acute as the opercula progressively overgrew the insula
and eventually met to form the closed Sylvian
fissure. As the temporal and parietal lobes enlarge they overgrow the insula (operculization). -
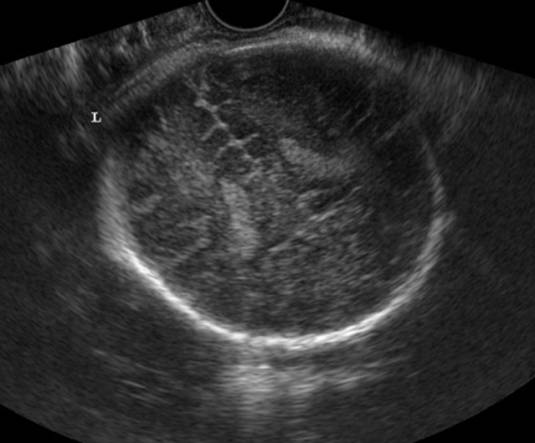
Acute insula / operculum angles are seen as early as 23.2 weeks
in some fetuses. -
After 24.5
weeks the angles were always acute. -
Anatomically, operculization can be seen by about 22-24 weeks (2,5,6). It begins at the posterior pointed end of the insula and proceeds anteriorly
(2,7). -
By 28-35
weeks, most of the insula is covered (1,7,8), but full closure of the most anterior part is not
achieved until birth to 2 years (9). -
The insular
plate remains smooth until insular sulci appear
anatomically starting about 32-35 weeks (1,9) at
which time they can also be recognized on MRI (10). This pattern of
development was also seen in the present study. As temporal and parietal operculization progressed, the angle between the insula and overgrowing brain changed from obtuse to
acute. An acute angle could be seen in some fetuses by 23.2 weeks and in
every fetus older than 24.5 weeks. |
||||||||||||||
|
|||||||||||||||
|
|
|
|
|||||||||||||
|
|
Earliest possible |
Latest not visible
Distinctly visible |
|||||||||||||
|
Convexity sulci |
23.2 |
25.5 27.8 |
|||||||||||||
|
|
|
||||||||||||||
|
26 |
Deepening of fissures and sulci. |
||||||||||||||
|
28-30 |
Growth spurt. Sulci and gyri |
||||||||||||||
|
|||||||||||||||
|
|
|
||||||||||||||
|
|
|
||||||||||||||
|
|
|
||||||||||||||
|
Ref: Toi A, Lister WS. How early are fetal
cerebral sulci visible and when can
lissencephaly be suspected. ISUOG
conference, |
|||||||||||||||










|
REFERENCES |
- Chi JG, Dooling EC, Gilles
FH. Gyral development of the human brain. Ann Neurol
1977; 1: 86-93
- Dorovini-Zis
K, Dolman CL. Gestational development of brain. Arch Pathol Lab Med 1977; 101: 192-195.
- Bernard C, Droulle P, Didier F, Gerard H, Larroche
JC, Plenat F, Bomsel
F, Roland J, Hoeffel JC. Echographic aspects of
cerebral sulci in the ante- and perinatal period [in French]. J Radiol 1988; 69: 521-532
- Hadi HA.
Fetal cerebral maturation in hypertensive disorders of pregnancy. Obstet Gynecol
1984; 63: 214-219.
- Ruoss K, Lovblad K, Schroth G, Moessinger AC, Fusch C.
Brain development (sulci and gyri)
as assessed by early postnatal MR imaging in preterm and term newborn
infants. Neuropediatrics
2001; 32: 69-74
- Patriquin
H, Fontaine S, Michaud J, Lafortune M, Boisvert J. Development of the fetal brain in the
second trimester: an anatomic and ultrasonographic
demonstration. Can Assoc Radiol J 1992; 43: 131-137.
- Monteagudo
A, Timor-Tritsch IE. Development of fetal gyri, sulci and fissures: a transvaginal sonographic study. Ultrasound Obstet
Gynecol 1997; 9: 222-228
- Chen CY,
Zimmerman RA, Faro S, Parrish B, Wang Z, Bilaniuk
LT, Chou TY. MR of the cerebral operculum: abnormal opercular
formation in infants and children. AJNR
Am J Neuroradiol 1996; 17: 1303-1311.
- Naidich
TP, Grant JL, Altman N, Zimmerman RA, Birchansky
SB, Braffman B, Daniel JL. The developing
cerebral surface. Preliminary report on the patterns of sulcal and gyral
maturation - anatomy, ultrasound, and magnetic resonance
imaging. Neuroimaging Clin N Am
1994; 4: 201-240.
- Levine D,
Barnes PD. Cortical maturation in normal and abnormal fetuses as assessed
with prenatal MR imaging. Radiology
1999; 210: 751-758.