|
DUCTUS VENOSUS
WAVEFORM |
During atrial contraction, foramen ovale is closed, and flow in the ductus venosus reflects the pressure gradient towards the RA, which in turn is dependent on a gradient between RA and RV.
About 50% of umbilical venous blood enters the ductus venosus and accounts for 98% of blood flow through it (portal blood is directed almost exclusively to the right lobe of the liver).
- Sampling site.
Velocities at the inlet of the ductus are higher than at the outlet into the IVC. Sample at the inlet to standardize. - Peak Velocities.
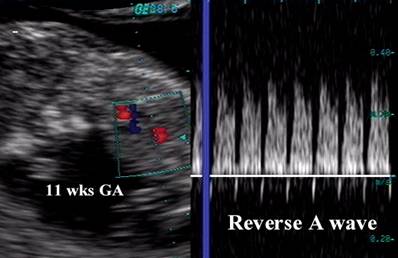
11-12 weeks GA = 20-30 cm/sec. Term 75cm/sec. The high velocity results in a jet of blood that has a tendency not to mix with IVC blood by preferentially directing it towards the foramen ovale and left atrium. Doppler demonstrates an abrupt change from non-pulsatile flow that is seen in the umbilical vein into a pulsatile flow pattern in the ductus. Absolute velocities can be recoded by pulsed doppler, but care must be taken to keep the angle of insonation below 30 degrees. - Waveform.
Has a triphasic pulsatile pattern. - I = begins with atrial relaxation and reaches a peak during ventricular systole.
- II = rapid filling phase of early diastole.
- III = reverse flow in late diastole due to atrial contraction. This reverse flow coincides with reverse flow seen in the IVC, however it never reverses completely (some flow is always present in the normal fetus). In healthy fetuses a significant reversal of the flow during atrial contraction is present with advancing gestation. The amount of reverse flow is directly proportional to the pressure gradient in the RA and RV at the end of diastole. This is also referred to as the A wave.
|
|
Video clip of the
Ductus Venosus Waveform
|
|
|
|
|
|

- Increased absolute
velocities reflect increased umbilicocaval (portocaval) pressure gradient
which may be caused by:
- Hypoxic
challenge, with a normal placental circuit (fetal exercise or anemia).
- Arterio-venous
fistula of the umbilical circuit or liver.
- Fetal
liver disease (parenchymal; infectious such as CMV; lymphoproliferative
disorders such as Down syndrome; tumors or other infiltrates).
- Increased
pulsatility is usually associated with altered cardiac function. One may
see a small or reversed A wave (III) from abnormalities of atrial
contraction. This may be due to:
- Increased
end-diastolic filling in congestive heart failure (Frank-Starling curve).
- Increased
end-diastolic filling caused by bradycardia (e.g. bradyarrhythmia,
AV-block).
- Increased
adrenergic drive (hypoxemia, increased afterload).
- Abnormal
atrial activity (supraventricular tachycardia).
- Myocardiopathies
or cardiac tumors.
- Tricuspid
or mitral incompetence.
- Cardiac malformations.
|
|
|
|
|
Absent A wave
|
|
|
Reverse A wave
|