|
NORMAL EMBRYOLOGY OF
BOWEL NORMAL PHYSIOLOGICAL
HERNIATION OF BOWEL |
- At about the fourth week of development, the primordial gut is closed at both the cranial and caudal ends by the oropharyngeal and cloacal membranes.
- The primordial gut forms as the flat, trilaminar embryonic disc goes through the process of median and horizontal plane infolding, pulling a portion of the yolk sac along with it.
- At this point, there are simultaneous events that further differentiate this originally featureless tube into their final, familiar forms.
o Formation of the tracheal bud along with infolding and fusion of the tracheoesphageal folds separate the trachea from the esophagus.
o There is asymmetric enlargement and rotation of the distal part of the foregut to form the embryonic stomach.
o The duodenum forms from a combination of the distal-most foregut and proximal midgut, is pulled along with rotation of the stomach, and goes through a normal period of temporary obliteration because of proliferation of its epithelial cells.
o The jejunum, ileum, and a large portion of the colon are derived from the midgut. During the period of rapid growth of the midgut, there is a normal herniation of bowel into the proximal portion of the umbilical cord. This occurs at the sixth week of development and lasts until about the tenth week when the intestines return to the embryonic abdomen. As the intestines return to the abdominal cavity, they undergo a 180° counterclockwise rotation.
In the normal situation, rotation and posterior positioning of most of the duodenum and all of the ascending colon leads to absorption of their mesenteries such that these structures become retroperitoneal. Finally, the distal colon and rectum are derived from the hindgut. The urorectal septum separates the urinary tract from the rectum.[
ANATOMY
|
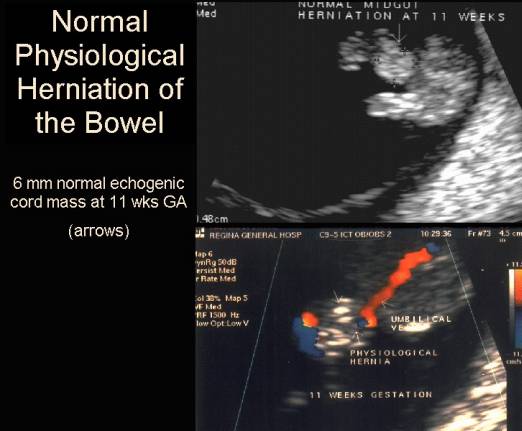
- Midgut grows faster than embryo, and herniates into base of cord (week 6), due to relative shortage of intra-abdominal space.
- Returns to abdomen by 12 weeks.
- The intestinal tract is a continuous tubular structure consisting of:
- Foregut - supplied by celiac artery.
- Midgut - supplied by superior mesenteric artery (SMA).
- Hindgut - supplied by inferior mesenteric artery (IMA).
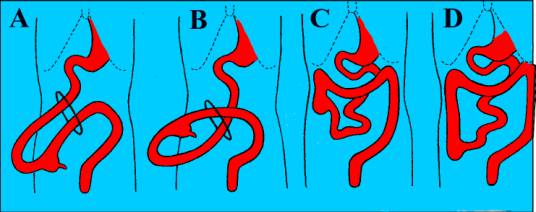
A – Prior to 6 weeks the duodenum rotates 900 counterclockwise and lies to the right of the SMA. The cecum rotates 900 counterclockwise and lies to the left of the SMA.
B – The duodenum rotates another 900 counterclockwise and lies posterior to the SMA. The rest of the midgut is in the umbilical cord.
C - <10-12 weeks, the intestines return to the peritoneal cavity. The final 900 counterclockwise rotation of the duodenum, with the duodeno-jejunal flexure lying to the right of the midline. The cecum rotates 1800. The right colon is the last portion of the GI tract to rotate completely, allowing the cecum to descend into the right lower quadrant.
D – The final stage is peritoneal fixation of
bowel. The small bowel mesentry is normally broad based with attachment extending
from the ligament of Treitz to the ileocecal valve. This broad base prevents
the small bowel from twisting around the SMA.
ULTRASOUND
|
Solid " mass" of mid to
high level echogenicity in the base of the umbilical cord, adjacent to the
fetal anterior abdominal wall.
|
|
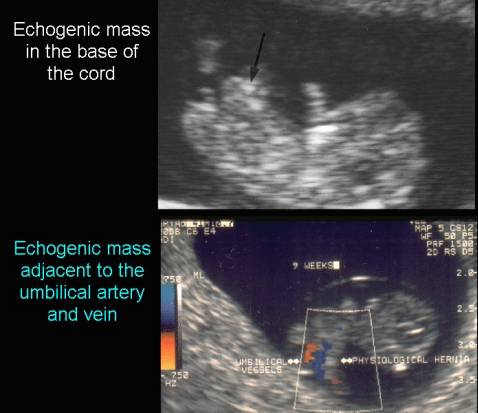
- Transverse and sagittal planes through fetal abdomen at level of umbilical cord.
- Measure longest and widest segment of cord.
- Echogenic mass:
- Normal cord mass = 4-7mm ( for a CRL of 19-44mm).
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|







- Abnormal cord mass.
- Cyr and associates - 5-10mm Mean 6.3mm
- Bowerman and associates - normal <7mm at any age. Any cord mass when CRL >44mm (11.1 weeks) is presumed abnormal.
- Normal cord with no mass = bright, parallel linear echoes due to specular reflections from external surface of walls of cord.
|
|
Video clip of
Physiological Hernia
|
|
|
|
|
|

- Three ultrasound forms have been described (1).
1. The cord is packed with intestinal loops.
2. Only a few intestinal loops remain herniated.
3. The last stage of herniation when only one loop of the cecum and adjacent jejunoileal loop remain inside the extraembryonic location.
Rotational
Abnormalities
|
||
Non Rotation |
Malrotation |
Reversed Rotation |
|
·
Midgut
returns to abdominal cavity after rotating only 1800 and not 2700. ·
Post-arterial
(colonic) limb reenters the abdominal cavity first instead of last. |
·
Rotation
occurs but is incomplete. ·
Prearterial
segment returns to the abdomen first and is usually in a normal position. |
·
Postarterial
segment of the midgut returns to the abdomen first. ·
This
unwinds the normal counterclockwise rotation that occurred during the first
stage and substitutes a final clockwise rotation of 900. |
|
·
Small
bowel on right side of abdomen. ·
|
·
Degree
of malrotation is indicated by position of cecum: ·
Cecum
may be on left side, higher than normal on the right side or in an
intermediate position. |
·
Transverse
colon lies behind the duodenum and is separated from it by the SMA. |
REFERENCES
|
- Bronshtein M, Yoffee N, Zimmer EZ. Transvaginal sonography at 5 to 14 weeks gestation: Fetal stomach, abnormal cord insertion, and yolk sac. Am J Perinatol 1992;9:344-347.
- Achiron R, Soriano D, Lipitz S et.al. Fetal midgut herniation into the umbilical cord: Improved definition of ventral abdominal anomaly with the use of transvaginal sonography. Ultrasound Obstet Gynecol 1995;6:256-260.