|
SIRENOMELIA |
Sirenomelia is a rare congenital abnormality characterized by a variety of anomalies involving the lower limbs, severe oligohydramnios that is secondary to the usually present bilateral renal agenesis, anorectal atresia and aberrant fetal vasculature. The antenatal diagnosis and differentiation from isolated bilateral renal agenesis is severly limited by the accompanying oligohydramnios that limits visualization of fetal anatomy.
Differentiation from true caudal regression syndrome is based on the belief that sirenomelia has a specific pathogenic factor (arterial steal), whereas caudal regression syndromes a heterogeneous group with diabetic embryopathy as the single most frequent etiological factor. This belief is compounded by reports of sirenomelia in infants of diabetic mothers (0.5-3.7% of cases of sirenomelia occurred in offspring of diabetic mothers)(2-3). Experimental studies by Alles and Sulik (4) produced caudal dysgenesis in mouse embryos by exposing them to etretinate (a synthetic vitamin A analogue and potent teratogen) on the eight day of gestation. Wei and Sulik (5) produced sirenomelia, secondary to cell death on the caudal mesoderm, in chick embryos exposed to ochratoxin (fungal toxin) during embryogenesis.
Prevalence - 1.5-4.2/100,000 live births (2). Male:Female ratio of 3:1.
PATHOGENESIS |
Vascular hypoperfusion is the favored theory (6). It is thought that a single large artery assumes the function of the umbilical arteries and diverts blood flow from the caudal portion of the embryo to the placenta, producing nutritional deprivation and maldevelopment of caudal structures. All infants appear to have a single umbilical artery (2).
The single lower extremity results either from failure of cleavage of the lower limb bud (1) or from the posterior fusion of the hindlimb primordia (7). Other workers (8 believe that neural tube overdistention in the caudal area leads to lateral mesodermal rotation, resulting in fusion of the lower limb buds and closure of the midline primitive gut and urethra.
An alteration in early vascular development results in a “vitelline
artery steal” (1) – blood from the caudal region of the embryo is
directed to the placenta resulting in multiple lower limb defects (lower somites do not develop due to the lack of perfusion). In
most cases the umbilical artery arises as an aberrant vessel from the old
vitelline arteries (superior mesenteric artery) or directly from the aorta.
CLASSIFICATION |
ULTRASOUND |
- Cranium and CNS:
- Usually normal.
- Face – Potter facies due to renal agenesis.
- Spine:
- Abnormality of the lower spine with varying degrees of involvement of the thoracic, lumbar and sacral spine. The spine may be difficult to accurately assess due to the profound oligohydramnios that may be present.
- Renal agenesis or dysgenesis. Multicystic kidneys have been described.
- Genitourinary system anomalies: agenesis of the genitourinary tract, no external genitalia or ambiguity.
- Single aberrant umbilical artery – Stevenson et.al. (1) proposed the “vitelline artery steal” theory. They reported that in each of 11 sirenomelic specimens, whom they had studied, a large artery, presumably a derivative of the vitelline artery arose from the aorta high in the abdominal cavity. Beyond this point the aorta and its branches are hypoplastic.
- Skeletal:
- Abnormality varies from simple cutaneous fusion of the limbs to complete absence of all long bones except for one femur.
- As the legs are fused, rotation is not possible and they retain their fetal position.
- Fibulae – when present they are between the tibia and sole of the foot (orientated ventrally instead of dorsally).
- Feet – The defects in the feet are proportional to the defects of the long bones. They range from a double fused foot with 10 toes to more severe defects presenting with a rudimentary foot and ectromelia.
- Gastrointestinal abnormalities:
- Absent / imperforate anus.
- Omphalocele.
- Small bowel duplication or short colon.
- Severe oligohydramnios / anhydramnios due to the lethal renal anomalies.
|
|
|
|
|
|
|
|

CASE REPORTS |
Over 20,000 routine obstetrical scans were performed over a 5 year period (January 1998 to January 2003) in our institution. Routine antenatal ultrasounds, including fetal echocardiograms were performed on all cases. All cases of severe oligohydramnios or anhydramnios were subjected to a targeted sonographic evaluation of the fetal vasculature and umbilical cord with color and / or power Doppler. Abnormal vasculature was diagnosed when either an abnormal vessel was noted in the abdomen coursing anteriorly to the umbilicus without passing lateral to the urinary bladder, or when the aorta ended abruptly or did not divide into two iliac arteries.
Three cases of sirenomelia were detected antenatally, 2 which underwent termination of pregnancy prior to 23 weeks of gestation, while one pregnancy proceeded to term after the couple received counseling. The presence of the abnormal fetal abdominal vasculature was determined antenatally, however the final mapping of the fetal vascular patterns were only obtained at pathological examination of the fetuses in 2 cases (Case 1 and 2), and in a one day old infant in the third case (Case 3).
The summary of the maternal history, sonographic findings and outcome are summarized in Table 1 and demonstrated in Figures 1-4.
Table 1. Maternal history, outcome and sonographic findings in three fetuses with sirenomelia.
|
|
Case 1 |
Case 2 |
Case 3 |
|
Maternal history |
No
drugs/diabetes |
No
drugs/diabetes |
No
drugs/diabetes |
|
Maternal age (yrs) |
21 |
33 |
27 |
|
GA of initial scan (wks) |
19 |
19 |
18 |
|
Classification |
Simelia apus (no feet) |
Simelia apus (no feet) |
Simelia dipus (two feet) |
|
Outcome |
TOP |
TOP |
Refused
TOP Demise
from renal insufficiency at 10 days of age |
|
Vertebral anomalies |
Sacral
dysplasia |
Sacral
agenesis |
None |
|
Pelvic anomalies |
Single
pelvic bone lying horizontally in pelvis |
|
None |
|
GI anomalies |
Blind
ending colon Anorectal atresia |
Blind
ending colon Anorectal atresia |
Hypoplastic
colon Imperforate
anus |
|
GUT anomalies |
Renal
agenesis |
Renal
agenesis |
Small
poorly functioning unilateral kidney |
|
Genital anomalies |
No
external genitalia |
No
external genitalia |
No
external genitalia |
|
Skeletal anomalies |
Single
blind ending femur No
tibiae or fibulae No
feet Heart-shaped
pelvic bone |
Single
blind ending femur No
tibiae or fibulae No
feet |
Two
femora (fusion of soft tissues) Two
tibiae (fusion of soft tissues) No
fibulae Two
feet |
|
CNS anomalies |
None |
None |
None |
|
Heart anomalies |
None |
None |
None |
|
Amniotic fluid |
Anhydramnios |
Anhydramnios |
Decreased
from 20 weeks until term |
|
Vascular anomalies: |
|
|
|
|
|
Hypoplastic
arising from vitelline vessel |
|
|
|
Not
seen - ? technical |
|
|
Absent |
Absent |
Hypoplastic
but present |
|
Absent |
Absent |
Hypoplastic
– patent left renal artery |
|
Single
left iliac artery as a continuation of aorta |
Single
left iliac artery arising as branch of vitelline vessel |
Two
iliac arteries from distal aorta |
|
Single
non-branching vessel terminating as left iliac artery |
Small
hypoplastic artery (only patent for 1cm distal to origin) |
Well
formed - slightly smaller than vitelline vessel Single
small renal artery arises from left side |
|
Large
dominant vessel No
branches |
Single
midline vessel coursing down to pelvis Celiac
artery arises from this vessel A
single left iliac artery arises from its distal portion |
Large
artery arises from aorta just distal to origin of celiac artery and SMA Coursed
through abdominal cavity on a short mesentery to umbilicus No
branches |
|
2
vessel cord |
2
vessel cord |
2
vessel cord |
Figure 1: Case 1 – Sirenomelia apus at 19 weeks of gestation.
- Anhydramnios with poor visualization of fetal anatomy.
- Color flow imaging of the umbilical cord demonstrating a single umbilical artery.
- Transverse scan through the fetal upper abdomen demonstrating bilateral renal agenesis.
- Color flow image through the fetal abdomen demonstrating Aberrant origin of umbilical artery (vitelline vessel) traversing anteriorly to the umbilicus. Note the absent relationship between the vitelline vessel and the expected position of the fetal bladder
- Post abortion specimen demonstrates a single femur and hypoplastic tibia.
|
a. |
b. |
|
|
|
|
c. |
d. |
|
|
|
|
e |
|
|
|
|



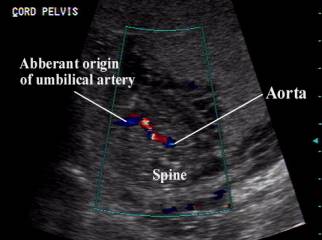

Figure 2: Case 2 – Simeia apus at 19 weeks of gestation.
- Blind ending single femur with complete anhydramnios.
- Poor visualization of normal fetal anatomy due to the anhydramnios.
- Sagittal color flow views of the fetus demonstrating a large aberrant vessel extending anteriorly with a small hypoplastic abdominal aorta which terminates abruptly just distal to the origin of the aberrant vitelline vessel.
- Post abortal radiograph demonstrating a single, blind ending femur and an abnormal heart shaped pelvic bone.
|
a. |
b. |
|
|
|
|
c. |
d. |
|
|
|


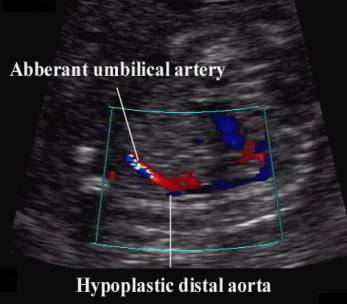


Figure 3: - Case 3 – Simelia dipus at 18 weeks of gestation.
- Gray scale image demonstrating two normal femora with soft tissue fusion centrally.
- This appearance is confirmed on the post natal image on day 1.
- Gray scale image demonstrating fusion of the feet at the heels with a relatively normal amount of amniotic fluid around the feet from the single functioning kidney.
- Color flow image demonstrates the abnormal vitelline vessel arising from the abdominal aorta and coursing anteriorly into the umbilical cord.
- Power doppler image in a sagittal plane demonstrates a normal caliber aorta (Ao) which bifurcated into two normal common iliac arteries. The aberrant vitelline artery (Vitt) originates anterior to the aorta and traversed the abdominal cavity and exited the fetal abdomen at the umbilicus as the single umbilical artery. The caliber of the vitelline artery is only slight smaller than the aorta.
- Infant on Day 1. The absent Potters facies is due to the small amount of amniotic fluid that was present throughout the pregnancy from the one poorly functioning kidney. Note the soft tissue fusion of the upper legs and the absent anus.
|
a + b |
|
|
|
|
|
c+d |
|
|
|
|
|
e |
|
|
|
|
|
|
|
|
f |
|
|
|
|
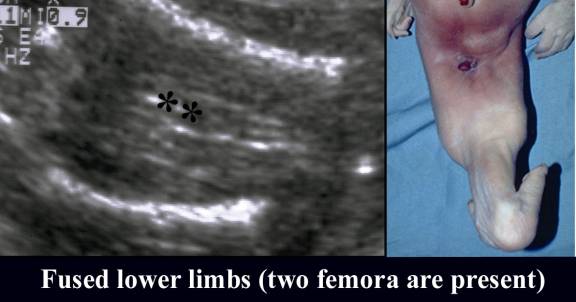




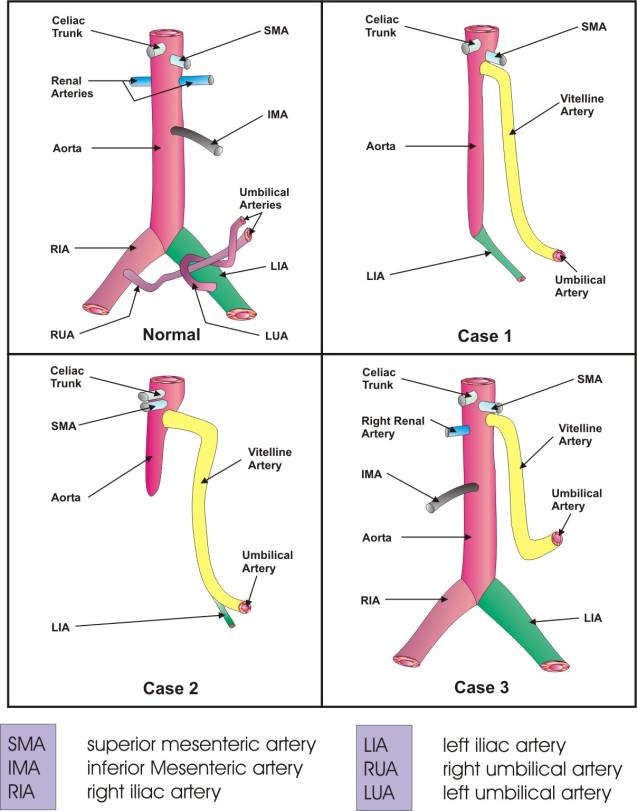
Figure 4. Vascular patterns associated with Sirenomelia in a normal fetus and in cases 1, 2 and 3.
Comparison
Of Sirenomelia And Caudal
Regression Syndrome
ASSOCIATED ANOMALIES |
- The association between sirenomelia and maternal diabetes is much less pronounced (2 of 80 cases in one series) (2).
- Monozygotic twinning (9-15% of cases). There is a 100-150 fold increased incidence of sirenomelia (7,9) when compared to dizygotic twins or singletons..
- Bilateral renal agenesis.
- Oligohydramnios.
- Lower vertebral/sacral defects.
- Single umbilical artery.
- Imperforate anus (10).
- Agenesis of the genitourinary system (11).
- Omphalocele (10).
- Scoliosis and malformed thorax (10).
- VACTERL association – some authors have demonstrated similarity in the phenotypic manifestations of sirenomelia and VACTERL sequences. In the series of Stoker and Heifetz (2), all 80 fetuses with sirenomelia had at least three other VACTERL anomalies, excluding the simpus (single lower limb). Duncan et.al. (3) demonstrated at least three of six VACTERL anomalies in 48 of the 50 sirenomelic fetuses. It appears that in most cases, the difference between sirenomelia and VACTERL sequences lies in the severity of the compartment defects, with the single lower limb being the classical sign in sirenomelia.
DIFFERENTIAL DIAGNOSIS |
REFERENCES |
- Stevenson RE, Jones KL, Phelan MC et.al. Vascular steal: The pathogenetic mechanism producing sirenomelia and associated defects of the viscera and soft tissues. Pediatrics 1986;78:451.
- Stocker JT, Heifetz SA. Sirenomelia. Perspect Pediatr Pathol 1987;10:7.
- Duncan PA, Shapiro LR, Klein RM. Sacrococcygeal dysgenesis association. Am J Med Genet 1991;411-53
- Alles AJ, Sulik KK. A review of caudal dysgenesis and its pathogenesis as illustrated in an animal model. Birth Defects 1993;29:83-102.
- Wei X, Sulik KK. A review of caudal dysgenesis / sirenomelia induced by ochratoxin A in chick embryos. Teratology 1996;53:378-391.
- Hoyme HE. The pathogenesis of sirenomelia: An editorial comment. Teratology 1988;38:485.
- Davies J, Chazan E, Nance WE. Symmelia in one of monozygotic twins. Teratology 1971;4:367.
- Gardner NJ, Breuer AC. Anomalies of heart, spleen, kidneys, gut and limbs may result from an overdistended neural tube. A Hypothesis. Pediatrics 1980;65:508.
- DiLorenzo M, Brandt ML, Veilleux A. Sirenomelia in an identical twin: A case report. J Pediatr Surg 1991;26:1334.
- Sirtori M, Ghidini A, Romero R et.al. Prenatal diagnosis of sirenomelia. J Ultrasound Med 1989;8:83-88.
- Brookshire-Quinn C, Jeanty P. Prenatal sonographic detection of symelic bipodia sirenomelia. JDMS 1990;2:103-105.