|
PIERRE ROBIN ANOMALAD
/ SYNDROME |
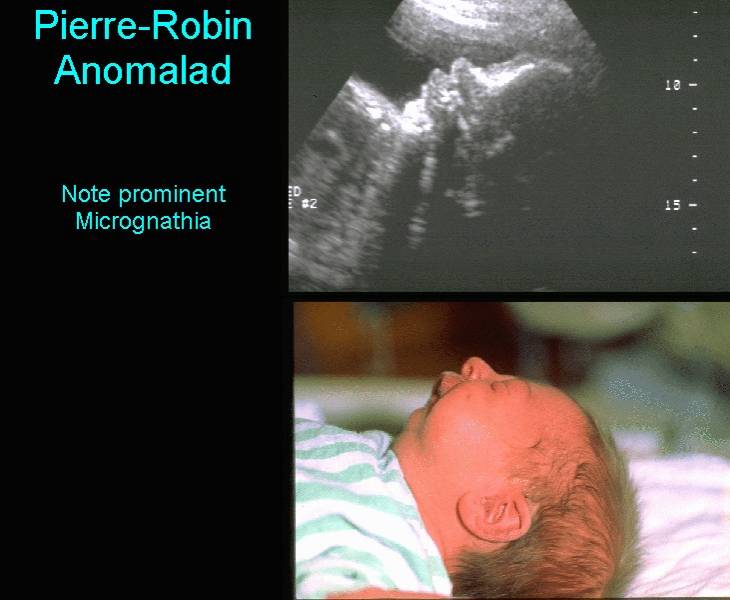
Robin sequence previously known as Pierre Robin syndrome and Pierre Robin anomalad consists of three essential components:
- Micrognathia or retrognathia
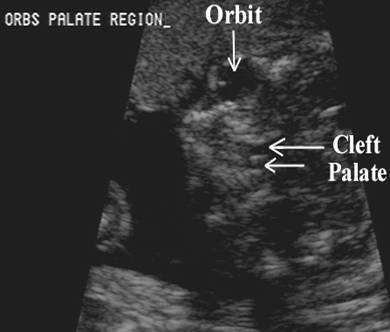
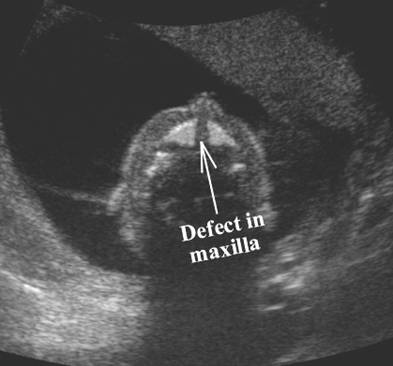
- Cleft palate (usually U-shaped, but V-shape also occurs)
- Glossoptosis (often accompanied by airway obstruction).The tongue is not actually larger than normal, but because of the small mandible, it is large for the airway and causes obstruction. Rarely, it can be smaller than normal.
Prevalence: 1:30,000.
Abnormal karyotypes in 10% of cases (14).
ULTRASOUND |
Pierre Robin syndrome is classified as a first branchial arch syndrome (1). Most cases are sporadic, however there are reported familial cases associated with several syndromes.
- Micrognathia.
- Cleft palate (U-shaped and not V-shaped).
- Glossoptosis.
- Ear defects.
- Eye defects.
- Cardiac anomalies (20%) (15).
|
Case
1 |
|
|
|
|
|
Case
2 |
|
|
|
|
|
|
Micrognathia |
|
|
Normal upper and lower lip |
|
Cleft
palate |
|
|
|
|
|
Case 3 |
|
|
|
|
|
|
|
|
|
|










ETIOLOGY / PATHOGENESIS |
Robin sequence (RS) is etiologically heterogenous. Etiologic heterogeneity suggests pathogenetic heterogeneity and phenotypic variability. These include various causes of malformations and deformations, and connective tissue dysplasia (see in details in the next Section). A major distinction should be made between isolated occurrences of Robin sequence and cases in which RS is part of a recognized syndrome, or part of a complex of multiple anomalies or an unrecognized syndrome.
Isolated RS is often a deformation resulting from intra-uterine forces acting on the mandible, which restrict its growth and impact the tongue between the palatal shelves. Some deformational cases of RS have been associated with oligohydramnios. The most severe cases of micrognathia are unlikely to be isolated RS caused by deformation.
The proportion of cases that are isolated varies in different studies.
· Hanson and Smith (1975) found that 25% of RS cases had specific syndromes, another 35% had multiple anomalies without a specific recognized syndrome, and only 40% had isolated RS.
·
Williams et al (1981) found that 74% of RS cases
were isolated. Among syndromic cases, the most common
is Stickler’s syndrome which makes up 20-25 % of all RS cases.The second most common RS syndrome is Velocardiofacial syndrome, about 15% of all RS cases (Shprintzen, 1981). Treacher
Collins syndrome, Nager syndrome, spondyloepiphyseal
dysplasia congenita, and
other recognized syndromes make up the rest of the syndromic
RS cases.
·
Cohen (1997) listed 46 conditions associated
with RS. When a diagnosis of RS is made, a full genetic evaluation (including
FISH for 22q deletion, test for mutation in Treacle(TCOF1)
gene) is appropriate, together with diagnostic tests for other suspected
syndromes (skeletal X-Rays, ophthalmology exam, etc.).
ASSSOCIATED SYNDROMES |
- about 40% of infants with Pierre Robin have Stickler Syndrome.
- Stickler Syndrome may
be the most common tissue disorder in the
- some degree of cleft palate
- cataracts and/or retinal detachment at an early age
- flat face
- Micrognathia
- skeletal abnormalities
- about 15% have Velocardiofacial Syndrome.
- also known as VCFS or as Shprintzen Syndrome, is the most common syndrome associated with cleft palate. Approximately 1 in 2,000-5,000 children are born with VCFS.
- a long face with a prominent upper jaw
- flattening of the cheeks
- an underdeveloped lower jaw
- a bluish color below the eyes
- a prominent nose with narrow nasal passages
- a long thin upper lip and a down-slanting mouth
- cleft palate or submucous cleft palate
- multiple abnormalities of the heart
- learning disabilities in one or more areas
- hearing loss
- problems with speech
- leg pain
- extremes of behavior
- Beckwith-Wiedemann
Syndrome
- CHARGE Syndrome
- DiGeorge
Syndrome
- Fetal Alcohol Syndrome
- Mandibulofacial
Dysostosis (Treacher
Collins Syndrome)
REFERENCES |
- Pilu G, Romero R, Reece EA et.al. The prenatal diagnosis of Robin anomalad. Am J Obstet Gynecol 1986;154:630-632.
- Chemke J, Carmi R, Galil A et.al. Weissenbacher-Zweymuller syndrome. A distinct automosomal recessive skeletal dysplasia. Am J Med Genet 1992;43:989-993.
- Beighton
P, Beighton G: The man behind syndrome.
- Bixler D, Christian JC: Pierre Robin syndrome occurring in two unrelated sibships. Birth Defects Orig Art Ser 1971; VII/7: 67-71.
- Cohen MM Jr:
Dysmorphology, syndromology,
and genetics in plastic surgery. In: McCarthy JG, ed. Plastic Surgery.
- Cohen MM Jr: Editorial comment. Robin sequences and complexes. Causal heterogeneity and pathogenetic/phenotypic variability. Amer J Med Genet 1999; 84: 311-315.
- Cohen MM Jr: Etiology and pathogenesis of orofacial clefting. Oral and Maxillofacial Surgery Clinics of North America 2000; 12/3: 379-397.
- Lehman JA, Fishman JRA, Neiman GS: Treatment of cleft palate associated with Robin sequence: Appraisal of risk factors. Cleft Palate Craniofac J 1995; 32: 25-29.
- Poswillo D: The aetiology and surgery of cleft palate with micrognathia . Ann R Coll Surg Engl 1968; 43(2): 61-88.
- Shah CV, Pruzansky S, Harris WS: Cardiac malformations with facial clefts; with observations on the Pierre Robin syndrome. Am J Dis Child 1970 Mar; 119(3): 238-44.
- Sheffield LJ, Reiss JA, Strohm K, Gilding M: A genetic follow-up study of 64 patients with the Pierre Robin complex. Amer J Med Genet 1987; 28: 25-36.
- Shprintzen Cleft Palate Craniofac J 1992; 29: 224- RJ: Pierre Robin, micrognathia, and airway obstruction: The dependency of treatment on accurate diagnosis. Int Anesthesiol Clin 1988; 26: 64-71.
- Smith JW, Stowe WR: The
Pierre Robin syndrome (glossoptosis, micrognathia, cleft palate). A review of 39 cases with
emphasis on associated ocular lesions. Pediatrics 1961; 27: 128-133.
- Teoh
M M, Meagher S. First trimester diagnosis of micrognathia as a presentation of
- Hsieh YY, Chang CC, Tsai HD et.al. the prenatal diagnosis
of Pierre Robin sequence. Prenat Diagn 1999;19:567-569.