|
ORAL CAVITY TUMORS
(1-7) |
|
Epulis (8) |
Benign granular cell tumor which is solid. It arises from the alveolar ridge. Color and power Doppler usually demonstrates marked blood flow in the tumor. It is a self limiting lesion and responds to conservative excision. |
|
Foregut duplication cyst (10) |
Enteric
duplication cyst may occur in the floor of the mouth. It is cystic in nature
and may closely mimic a ranula. |
|
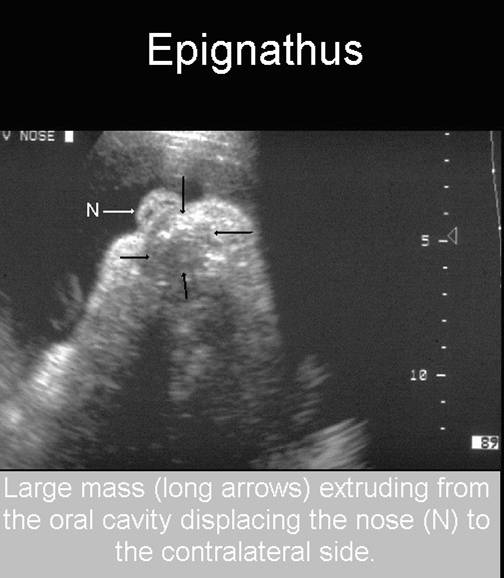
Epignathus (11,12) |
Oropharyngeal teratoma mostly arising from the palate. It appears as solid-cystic tumor with mixed areas of hypo and hyperechogenicity, may have calcifications and is found in association with polyhydramnios. It can cause significant morbidity and mortality |
|
Median palatal mucosal cyst [Epstein’s pearl] |
Benign and self resolving |
|
Vascular hamartomas (4,5) |
Hemangiomas or lymphangiomas [cystic hygromas] and are usually located on the tongue. These tumors may appear as solid- cystic masses on ultrasound and require surgical excision. |
|
Other tumors of the tongue (1-16) |
•
Thyroglossal duct cyst |
|
RANULA - RETENTION
CYST, MUCOCELE, ORAL PSEUDOCYST |
A congenital ranula is a cystic malformation seen in the oral cavity that usually results from the obstruction of the sublingual or minor salivary glands. These pseudocysts are normally located in the sub-lingual space between the mylohyoid muscle and the lingual mucosa.
PREVALENCE |
The incidence of a congenital ranula is estimated to be 0.74%.
ETIOLOGY |
A ranula is a fluid collection
that occurs either due to:
1. Disruption of minor salivary ducts leading to extravasation
of mucous structures into adjacent structure and resulting in a mucous extravasation cyst. These are more common in children and
young adults and rarely occur in neonates. The ranula
is not lined by an epithelium in this case.
2. A blocked duct causing proximal expansion and resulting in a mucous
retention cyst, seen in neonates and the fluid collection is lined by salivary
duct epithelium.
Types: Ranulas can be classified according to their site of location. They can be
• A simple ranula –
located in the floor of the mouth,
• A cervical ranula – located in the paracervical region,
• And a plunging ranula – located near
the upper airway and extending into the floor of the mouth. [plunging
ranulas exhibit a so called ‘tail sign’
on MRI].
ULTRASOUND |
• A hypoechoic cystic mass
in the floor of the mouth, with no solid components.
• If very large, the mass may displace the tongue upwards.
• No vascularity can be seen within this cystic
structure.
If the mass becomes too large, it may interfere with swallowing resulting in polyhydramnios.
REFERENCES |
1. Shipp TD, Bromley B, Benacerraf B. The ultrasonographic appearance and
outcome for fetuses with masses distorting the fetal face. J Ultrasound
Med. 1995 Sep; 14(9):673-8.
2. Fernandez Moya JM, Cifuentes
Sulzberger S, Diaz Recasens J, et al. Antenatal
diagnosis and management of a ranula. Ultrasound Obstet Gynecol. 1998 Feb;
11(2):147-8.
3. Onderoglu L, Saygan-Karamursel
B, Deren O, et al. Prenatal diagnosis of ranula at 21 weeks of gestation. Ultrasound Obstet Gynecol. 2003 Oct;
22(4):399-401.
4. Rousseau T, Couvreur S, et al. Prenatal diagnosis
of enteric duplication cyst of the tongue. Prenat Diagn. 2004 Feb; 24(2):98-100.
5. Akyol MU, Orhan D.
Lingual tumors in infants: a case report and review of the literature. Int J Pediatr Otorhinolaryngol.
2004 Jan; 68(1):111-5.
6. Jorgenson RJ,
7. Polak P, Santavy J, Micanik B, et al. An unusual tumor of the
oral cavity in a fetus and prenatal ultrasonography--case
report. Ceska Gynekol.
2002 May; 67(3):163-7.
8. Nakata M, Anno K, Matsumori
LT, et al. Prenatal diagnosis of congenital epulis: a
case report. Ultrasound Obstet Gynecol.
2002 Dec; 20(6):627-9.
9. Saheeb BD. Recurrent congenital bilateral ranula: a case report.
SADJ. 2001 Aug; 56(8):366-8.
10. Kong K, Walker P, Cassey J, O"Callaghan
S. Foregut duplication cyst arising in the floor of mouth. Int
J Pediatr Otorhinolaryngol.
2004 Jun; 68(6):827-30.
11. Morof D, Levine D, Grable
I, et al. Oropharyngeal Teratoma: Prenatal Diagnosis
and Assessment Using Sonography, MRI, and CT with
Management by Ex Utero Intrapartum Treatment Procedure.
AJR Am J Roentgenol. 2004 Aug; 183(2):493-6.
12. Gaucherand P, Rudigoz
RC, Chappuis JP. Epignathus:
clinical and sonographic observations of two cases.
Ultrasound Obstet Gynecol.
1994 May 1;4(3):241-4
13. Ikemura K, Kakinoki Y, Nishio K, Suenaga Y. Cysts of the
oral mucosa in newborns: a clinical observation. J UOEH.
1983 Jun 1; 5(2):163-8.
14. Lalwani AK, Engel TL. Teratoma of the tongue: a
case report and review of the literature. Int J Pediatr Otorhinolaryngol. 1992
Nov; 24(3):261-8.
15. Stevens GH, Schoot BC, Smets
MJ, et al. The ex utero intrapartum
treatment (EXIT) procedure in fetal neck masses: a case report and review of
the literature. Eur J Obstet
Gynecol Reprod Biol. 2002
Jan 10; 100(2):246-50.
16. Haberal I, Gocmen H, Samim E. Surgical management of pediatric ranula. Int J Pediatr
Otorhinolaryngol. 2004 Feb; 68(2):161-3.
|
EPIGNATHUS - TERATOMA OF ORAL CAVITY OR PHARYNX |
Epignathus is a congenital teratoma of the hard palate in the region of Rathke's pouch.
Incidence: 1:35,000 to 1:200000 live births.
PATHOLOGY (1,2) |
- Consist of tissue derived from any of the three germinal layers.
- Most contain adipose tissue, cartilage, bone and nervous tissue.
- Most are benign.
- Most are thought to arise from pluripotent cells in Rathke’s pouch that grow in a disorganized manner.
- Some arise from hard and soft palate, pharynx, tongue or jaw.
- They grow into the oral cavity, nasal cavity or intracranially from their sites of origin.
- They can completely occupy the mouth and airways and lead to rapid neonatal asphyxia unless they are recognized antenatally.
ULTRASOUND (2-5) |
- Solid tumor occupying the oral cavity and extending a variable distance out of the oral cavity.
- ± Calcifications.
- ± Cystic components.
- Polyhydramnios due to obstruction to fetal swallowing (poor prognosis).
- The tumor is usually unidirectional and extends into the oral cavity. Bidirectional epignathus has been reported (8) involving both the oral cavity and intracranial structures.
- Maternal serum alpha-fetoprotein may be elevated.
- Earliest diagnosis – 15 weeks (8). Most are diagnosed after 20 weeks.
|
|
|
|
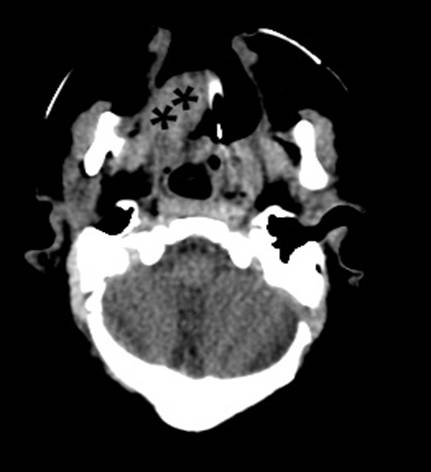
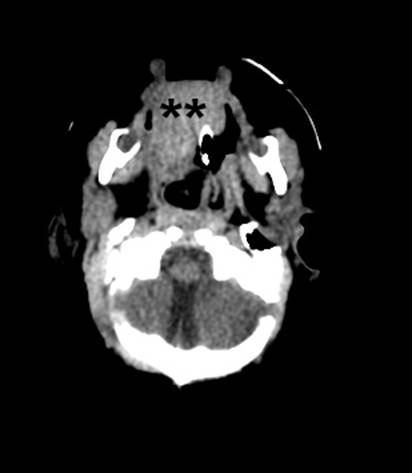
CT Scan on Day 1 |
|
|
|
|
|
|
|


ASSOCIATED ANOMALIES (2,6, 7) |
6% of fetuses have associated anomalies:
- Multiple facial hemangiomas.
- Cleft palate.
- Bifid tongue or nose.
- Branchial cysts.
- Hypertelorism.
- Umbilical hernia.
- Congenital heart defects.
- Chromosomal aberrations that have been associated include (10-12): 45,Xx/46,r(X) mosaicism; trisomy 13; duplication of 1q and 19 p; inverted proximal 1q duplication.
DIFFERENTIAL DIAGNOSIS |
- Teratomas of the neck.
- Cephaloceles.
- Conjoined twins.
- Other facial tumors (hemangioma, lymphangioma, neurofibroma and granular myoblastoma) (9).
REFERENCES |
- Carney JA, Thompson DP, Johnson CL et.al. Teratomas in children: Clinical and pathologic aspects. J Pediatr Surg 1972;7:271.
- Shah BL, Vasan U, Raye JR. Teratoma of the tonsil in a premature infant. Case report and review of the literature. Am J Dis CHILD 1979;133:79.
- Chervanek FA, Tortora M, Moya FR et.al. Antenatal sonographic diagnosis of epignathus. J Ultrasound Med 1984;3:235.
- Hawkins DB, Park R. Teratoma of the pharynx and neck. Ann Otol Rhinol Laryngol 1972;81:848.
- Kang KW, Hissong SL, Langer A. Prenatal ultrasonic diagnosis of epignathus. J Clin Ultrasound 1978;6:330.
- Fraumeni JF Jr, Li FP, Dalager N. Teratomas in children: Epidemiologic features. J Natl Cancer Inst 1973;51:1425.
- Wilson JW, Gehweiler JA. Teratoma of the face associated with a patent canal extending into the cranial cavity (Rathke's pouch) in a three week old child. J Pediatr Surg 1970;5:349.
- Gull I,
Wolman I, Har-Toov J et.al.
Antenatal sonographic diagnosis of epignathus at
15 weeks of pregnancy. Ultrasound Obstet Gynecol 1999;13:271-273.
- Meizner I, Shalev J, Mashiach R et.al. Prenatal ultrasonographic diagnosis of oral granular cell myoblastoma. J Ultrasound Med 2000;19:337-339.
- Witters I, Moerman P, Louwagie D et.al. Second trimester prenatal diagnosis of epignathus teratoma in ring X chromosome mosaicism with inactive ring X chromosome. Ann Genet 2001;44:179-182.
- Yapar EG, Ekici E, Gokmen O. Sonographic diagnosis of eopignathus, prosencephaly, meromelia and ligohydramnios in a fetus with trisomy 13. Clin Dysmorphol 1995;4:266-271
- Schwartz S, Raffel LJ, Sun CC et.al. An unusual mosaic karyotype detected through prenatal diagnosis with duplication of 1q and 19 p and associated teratoma development. Teratology 1992;46:399-404.