|
INTERRUPTED INFERIOR
VENA CAVA WITH AZYGOUS
CONTINUATION |
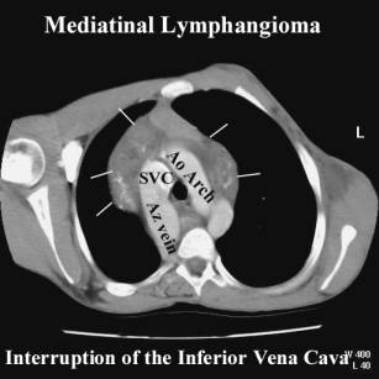
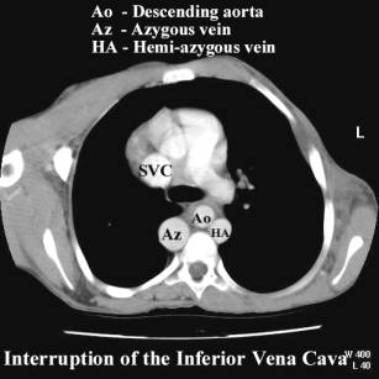
Interrupted inferior vena cava with azygous continuation is caused due to failure of connection between the right subcardinal vein and right vitelline vein. The result is that venous blood from the caudal part of the body reaches the heart via the azygous vein draining into the superior vena cava.
EMBRYOLOGY
|
Normally the right sacrocardinal, subcardinal and vietlline veins form the inferior vena cava (IVC) between the 5th and 7th weeks of gestation. These veins become the sacrocardinal, renal and hepatic segments of the IVC. Interruption of the IVC occurs when the right subcardinal vein fails to connect with the right vitelline vein. Venous blood is shunted directly into the right supracardinal vein (which later develops into the azygous vein).
ULTRASOUND
|
- Usually found in cardiosplenic syndromes:
- Polysplenia (85%) (1).
- Asplenia (less commonly) (2).
- May be isolated with normal outcome (3).
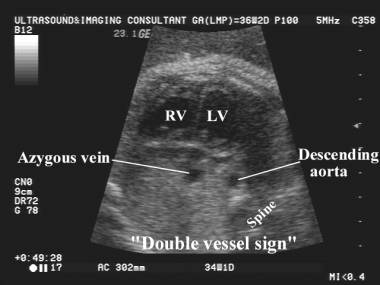
- Vessel parallel to the aorta (slightly smaller in caliber) on sagittal views.
- Double vessel sign on transverse (axial images) at the level of the heart (4).
- No intrahepatic portion of the IVC.
- Hepatic veins and ductus venosus are normal.
- Cardiac and intra-abdominal abnormalities in cardiosplenic syndromes.
- No hemodynamic or pathological significance in the absence of associated cardiac anomalies.

|
ENLARGED / DILATED
INFERIOR VENA CAVA |
An enlarged inferior vena cava may be due to:
- Decreased (slow) flow within the vessel. This is usually due to obstructive lesions of the right side of the heart (atresia of the AV valve; endocardial cushion defect; univentricular heart, severe valvular dysplasia with regurgitation; atrial myxomas). There should be other signs of heart failure including ascites, dilated heart, abnormal flow velocity waveforms in Ductus and IVC).
- Increased flow in the vessel. This may occur to increased blood flow through a “shunt” that increases volume and flow in the IVC. The most common causes of this phenomenon are vein of Galen arterio-venous malformation; placental chorioangioma; hepatic angioma and hemangioendothelioma. Other causes of increased flow result from aberrant connection of the umbilical vein to the iliac vein (in cases of agenesis of the ductus venosus).
REFERENCES
|
- Van Praagh S, Santini F, Sanders SP. Cardiac malpositions with special emphasis on visceral heterotaxy (asplenia and polysplenia syndromes). In: Fyler DC (ed). Nadas Pediatric Cardiology. Philadelphia: Hanley and Belfus 1992;589-608.
- Ruscazio M, Van Praagh S, Marrass AR et.al. Interrupted inferior vena cava in asplenia syndrome and a review of the hereditary patterns of visceral situs abnormalities. Am J Cardiol 1998;81:111-116.
- Celentano C, Malinger G, Rotmensch S et.al. Prenatal diagnosis of interrupted inferior vena cava as an isolated finding: a benign vascular malformation. Ultrasound Obstet Gynecol 1999;14:215-218.
- Sheley RC, Nyberg DA, Kapur R. Azygous continuation of the interrupted inferior vena cava: a clue to prenatal diagnosis of cardiovascular syndromes. J Ultrasound Med 1995;14:381-387.