NON TROPHOBLASTIC PLACENTAL TUMORS
|
Chorioangioma - Teratoma - Metastasis
|
CHORIOANGIOMA (1-5) |
- The chorioangioma or placental hemangioma is the most common benign tumor of the placenta, followed by hydatidiform mole and choriocarcinoma..
- Most common non trophoblastic placental tumor and has a reported incidence of between 0.2‑139:10,000 births (Large tumors, those greater than 5 cm, have been reported to occur from 0.2‑4:10,000 births. Smaller chorioangiomas occur more frequently with an incidence of 14‑139:10,000 deliveries) (22,23).
- Reported incidence in pathological series is as high as 1%, however not all tumors are sonographically visible (24).
- The recurrence risk is not yet known but appears to be very small.
- Chorioangiomas are hamartoma, which arise as a malformation of the primitive angioblastic tissue of the placenta.
- Small tumors are essentially asymptomatic.
- Large, clinically significant chorioangiomas occur much less frequently, with a reported incidence ranging from 1 in 3500 to 1 in 9000 births.
- Large chorioangiomas (>5cm) are thought to act as peripheral arteriovenous shunts resulting in cardiac overload, complications associated with them include congestive heart failure, polyhydramnios, hydrops fetalis, premature labor, maternal and fetal coagulopathies and hemolytic anemia (5,8,40,41).
PATHOGENESIS
|
A chorioangioma originates from primitive chorionic mesenchyme. It develops when blood vessels and stroma proliferate independently of the surrounding tissue.
Marchetti (25) describes three histological tumor types (believed to represent various phases of tumor development)
· One type is less differentiated or more immature with a compact structure of mostly cellular elements.
·
The second type is the mature angiomatous or vascular type. This is the most common type
of chorioangioma composed of numerous small blood
vessels and capillaries.
·
The last type is characterized by degenerative
changes.
Although tumors tend to be of one type, some may exhibit a
combination of the characteristics described above.
Chorioangiomas are believed to originate at about the 16th day after fertilization, although there has been no documentation of chorioangiomas during the first trimester.
ULTRASOUND
|
The specific findings of chorioangioma are variable, and depend largely on the histological composition of the tumor (angiomatous, cellular or degenerative).
Histological classification correlates well with the sonographic features.
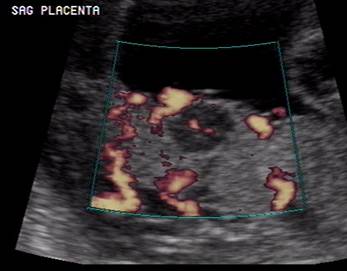
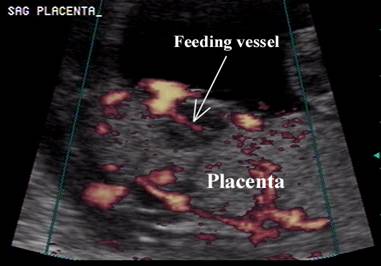
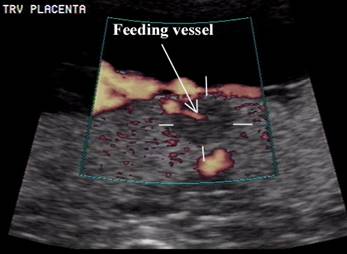
· If the mass is predominantly vascular, color flow imaging reveals a hypervascularization pattern.
·
Cellular and degenerative types are solid or
cystic tumors with little vascularity and the
gray-scale appearance ranges from echogenic to hypoechogenic.
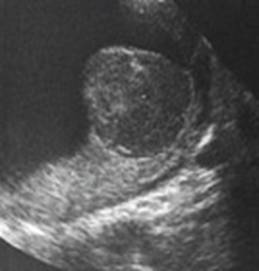
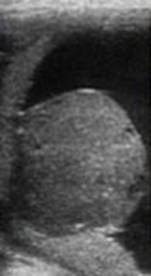
- Rounded, primarily hypoechoic or mixed echogenic mass. It is well circumscribed and has a different echogenicity from the rest of the placental tissue.
|
|
|
|
|
|


- Most chorioangiomas are small, single, circular, encapsulated and intraplacental. Ultrasound appearances that have been described include:
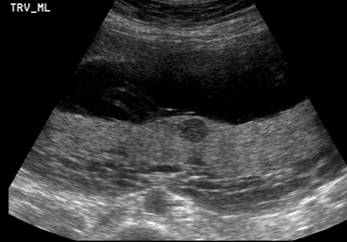
- Multicystic (12) – the case below demonstrates the rare multicentric angiomatous form (target lesions with hypoechoic central portion and echogenic rim). All lesions demonstrated peripheral arterial inflow and venous outflow on color doppler.
|
|
|
|
|
|




- Echogenic mass with dilated vascular channels (13).
- Complex (14,15).
- Uniformly and non-uniformly solid (16-18).
- Multitumoral (19).
- Usually situated near the
umbilical cord insertion site.
- They are surrounded by a
capsule or pseudocapsule.
- Location:
- These tumors are usually a single,
well-circumscribed mass within the placental substance, but they can
present as multiple separate masses that usually bulge into the amniotic
cavity.
- Less often they can be located in the membranes
and attached to the placenta by a vascular pedicle.
- They have also been described on the umbilical cord (22).
- Rarely they may present as diffuse mass lesions. Our case presented as “target lesions” with a hyperechogenic periphery and central hypoechoic central portion.
- Usually on the surface of the placenta.
- Usually 1-5 cm in size.
- Mild to moderate blood flow on color doppler (helps distinguish chorioangioma from an intraplacental hematoma).
- Non-immune hydrops (6), thought to be caused by shunting of blood through a large arteriovenous malformation (seen with large tumors)
- Calcification seen sonographically has not been reported (7).
- Polyhydramnios (14-33%) independent of tumor size and is probably related to the vascularity of the tumor and fluid leakage. Polyhydramnios and fetal hydrops may spontaneously regress when the chorioangioma degerates (8,20,21).
- Color doppler pattern is dependent on the histological type of the tumor. Cellular tumors consisting of mixed mesenchymal tissue are relatively avascular whereas the angiomatous type is vascular. Lesions above 7-8 cm may get shunting of fetal blood through the tumor (arterio-venous fistula). Janiaux and Ogle (8) suggest that vascularization of the tumor is an important determining factor of pregnancy outcome. No specific complications should be expected in avascular tumors whereas vascular tumors containing numerous large vessels may result in polyhydramnios and fetal congestive cardiac failure.
- CDI plays an essential role in the differential diagnosis and management of chorioangiomas. Where the tumor is avascular, no specific complications should be expected. Where the tumor is vascularized, and in particular if it contains numerous large vessels, serial ultrasound and Doppler examinations is warranted to detect fetal complications and polyhydramnios (8).
- Color Doppler imaging has contributed greatly to the prenatal differentiation between placental chorioangiomas and other nonvascular tumors such as hematoma, infarcts, intervillous thrombosis, teratoma and partial mole (42,43).
- The angioarchitecture revealed by 3D power Doppler confirms that the vascular channels in the tumor were continuous with the fetal circulation. This rules out other vascularized lesions such as placental hemorrhage (44), maternal lakes, degenerated myoma or placenta accrete (45,46).
- Using color Doppler ultrasound, Jauniaux and Ogle (47) categorized various vascular patterns of chorioangiomas and further identified that tumor vascularization is a pivotal determinant factor of pregnancy outcome.
- Hsieh and Soong (48) illustrated how changes on intracardiac Doppler, rather than a change in tumor size, could reflect the pathophysiological situation in the presence of a chorioangioma. However, detection of such subtle changes requires a high level of expertise.
|
|
|
|
|
|
|
|
|

- Pulsed doppler – waveform usually shows a typical fetal pattern.
- An increase in the echogenicity of the tumor as pregnancy advances is a good prognosis as this appearance is related to fibrotic degeneration of the lesion, reducing the amount of fetal blood shunted through the tumor (8).
COMPLICATIONS
|
- Chorioangiomas >5 cm are more frequently associated with fetal and maternal complications (hydrops, thrombocytopenia, elevated maternal serum Afp. Large tumors require 1-2 week serial ultrasounds to monitor growth and the development of hydrops.
- Fetal anemia with or without associated hydrops (7).
- Polyhydramnios - incidence of polyhydramnios has been found to be related to the size of the tumor. It occurs in 18‑35% of patients with large tumors (26).
- Oligohydramnios has been reported to be associated with chorioangioma. This diagnosis was made subjectively at the time of birth in a term gestation without the benefit of sonography. This association has not been confirmed by subsequent literature (27).
- Obstructed labor, which were attributed to the size and location of the chorioangioma (25). These reports have not been substantiated by more recent literature and appear to have been a coincidental rather than a causal finding.
- The incidence of preeclampsia is believed to be increased by some (23,28), but others (22,26,29) believe the incidence is similar to that of the general population. Froehlich, using ColLaborative Research Study data, has documented an increased incidence of preeclampsia of 16.4% vs 4.8% when comparing a group of 76 women with chorioangioma to a control group of 44,994 women (28).
- Antepartum
bleeding is believed to be caused by a premature separation of the
placenta as a result of bleeding from the tumor bed or a rupture of the
vascular pedicle.
- Froehlich reported a 4.0% incidence of abruptio placenta in the group with chorioangioma vs 1.2% in
the control group (28).
- Postpartum hemorrhage has been reported to
occur on occasions secondary to the over‑distension of the uterus
and subsequent uterine atony. Rarely the tumor
has been reported to remain in the uterine cavity after delivery of the
placenta and has caused postpartum hemorrhage (22).
- There is a case report of ovarian theca lutein cysts and high levels of hCG being associated with chorioangioma (30). The cause of these cysts is
unknown but may occur either as a result of high hCG levels or as an abnormal ovarian response to
normal hCG levels. The authors believe that the
source of hCG in their
case may be either the enlarged placenta or the chorioangioma
itself.
- Elevated serum alpha‑fetoprotein
levels associated with chorioangioma. It is
believed that this elevation is caused by feto‑maternal
hemorrhage.
- Arteriovenous
shunts have been reported in large chorioanfiomas,
which can result in fetal tachycardia, cardiomegaly
and hypervolemia (31). As a result, there
is the possibility of high output cardiac failure, edema, hydrops, and stillbirth (32-34). Fetal anemia can also
lead to hydrops through compensatory production
of red cells by the liver, which causes hepatomegaly,
portal hypertension, and hepatic cell dysfunction, resulting in hypoproteinemia.
- The abnormal tortuous vascular channels in these
tumors may cause red cell destruction and platelet sequestration,
resulting in thrombocytopenia, microangiopathic
hemolytic anemia, and disseminated intravascular coagulation (35). Feto‑maternal hemorrhage may also cause fetal
anemia (36,37).
- There appears to be a connection between chorioangiomas and other vascular anomalies
such as skin hemangiomas and single umbilical
artery. The incidence of single umbilical artery in pregnancies
complicated by chorioangioma is 2.7% compared to
0.7% in the control group, and the incidence of skin lesions is 12.2%
versus 2.1% in the control group (28).
- Although there have been some reports of chromosome
abnormalities associated with chorioangiomas (28,38,39), this does not seem to be a true association.
- Higher incidence of velamentous insertion of the cord (4.1% vs 1.5%) (28).
- Chazotte and colleagues (48) first reported a case of spontaneous infarction of a chorioangioma, which was evident from decreasing tumor size and gradual transition to an echolucent appearance on ultrasound.
DIFFERENTIAL DIAGNOSIS
|
- Placental hemorrhage may be sonographically indistinguishable (6). Placental hemorrhage may show some diminution in size over a period.
- Placental metastasis from a primary maternal tumor (very rare).
- Submucus fibroids – located on the maternal side rather than the placental side.
·
Partial hydatidiform moles
are characterized by localized swelling of chorionic villi with focal trophoblastic
hyperplasia and, on ultrasound, appear as multiple diffuse sonoluscent
intraplacental areas.
- Rare tumor.
- There is a controversy as to whether they actually arise from abnormal fetal development in a twin pregnancy. The distinction between placental teratoma and fetus amorphous (blighted fetus in a twin pregnancy) is controversial (9).
- Fox's criteria (10) - teratomas are characterized by a lack of development of skeletal parts and absence of an umbilical cord. Fox postulates that because germ cells are capable of multifarious differentiation and have migratory capabilities, they are able to implant at various sites and can develop into teratomas.
- During the first three months of fetal development, primordial germ cells migrate out through the wall of the envaginated gut into the umbilical cord. With further migrations these cells could land up in the placenta and thus form a nidus for placental teratoma. Therefore histological analysis is required to differentiate a teratoma from fetus amorphous (9).
ULTRASOUND
|
- Mixed cystic and solid masses that resemble a chorioangioma.
- 10-20% are purely cystic (10).
- Calcification occurs in 40% of cases.
|
|

|
PLACENTAL METASTASIS |
REFERENCES
|
- Spirit BA, Gordon L, Cohen WN et.al. Antenatal diagnosis of chorioangioma of the placenta. AJR 1980;135:1273.
- Dao AH, Rogers CW, Wong SW. Chorioangioma of the placenta: Report of 2 cases with ultrasound study in 1. Obstet Gynecol 1981;57:46S.
- O'Malley BP, Toi A, deSA DJ et.al. Ultrasound appearance of placental chorioangioma. Radiology 1981;138:159.
- Hadi HA, Finley J, Strickland D. Placental chorioangioma: Prenatal diagnosis and clinical significance. Am J Perinatol 1993;10:146.
- Hirata GI, Masaki DI, O'Toole M et.al. Color flow mapping and doppler velocimetry in the diagnosis and management of a placental chorioangioma associated with non immune fetal hydrops. Obstet Gynecol 1993;81:850.
- Bromley B, Benacerraf BR. Solid masses on the fetal surface of the placenta: Differential diagnosis and clinical outcome. J Ultrasound Med 1994;13:883-886.
- Haak MC, Oosterhof H, Mouw RJ et.al. Pathophysiology and treatment of fetal anemia due to placental chorioangioma. Ultrasound Obstet Gynecol 1999;14:68-70.
- Janiaux E, Ogle R. Color doppler imaging in the diagnosis and management of chorioangiomas. Ultrasound Obstet Gynecol 2000;15:463-467
- Williams VL, Williams RA. Placental teratoma: Prenatal ultrasonographic diagnosis. J Ultrasound Med 1994;13:587-589.
- Fox A. Pathology of the
human placenta. In: Fox H: Major problems in pathology. Vol. 7.
- Weinraub Z, Gembruch U, Forisch HJ et.al. Intrauterine mediastinal teratoma associated with non-immune hydrops fetalis. Prenat Diagn 1989;9:369.
- Seifer KDB, Ferguson JE, Bechren CM et.al. Non-immune hydrops fetalis in association with hemangiomata of the umbilical cord. Obstet Gynecol 1985;66:283-286.
- Grundy HO, Byers L, Walton S et.al. Ultrasonographic features and management of placental chorioangioma. J reprod Med 1986;31:520-522.
- Asokan S, Chadalavadu K, Gardi R et.al. Prenatal diagnosis of placental tumor by ultrasound. J Clin Ultrasound 1978;6:180-181.
- van Werring JH, van der Slikke JW. Prenatal diagnosis of chorioangioma associated with polyhydramnios using ultrasound. Eur J Obstet Gynae Reprid Biol 1985;19:255-259.
- Spirt BA, Gordon L, Cohen WN et.al. Antenatal diagnosis of chorioangioma of the placenta. Am J Roentgen 1980;135:1273-1275.
- Dao AH, Rogers CW, Wong SW. Chorioangioma of the placenta: Report of two cases with ultrasound study in one. Obetet Gynecol 1981;5746S-49S.
- Zalev AH. Placental chorioangioma, an unusual cause of polyhydramnios: Antenatal diagnosis. J Can Assoc Radiol 1986;37:60-61.
- Arodi J, Auslende R, Atad J et.al. Giant chorioangioma of the placenta. Acta Obstet Scand 1985;64:91-92.
- Chazotte C, Griz B, Koenigsberg M et.al. Spontaneous infarction of placental chorioangioma and associated regression of hydrops fetalis. Am J Obstet Gynecol 1990;163:1650-1658.
- MacIntosh
AM, Osborn RA. Chorioangioma
of the placenta: report of a case associated with spontaneous reabsorption of an acute hydramnios.
Med J Austral 1968;2:313-314.
- Fox H. Vascular tumors of
the placenta. Obstet Gynecol
Surv 1967;22:697‑711.
- Wentworth P. The incidence
and signifance of hemangioma
of the placenta. J
- Lopez HB, Kristoffersen SE. Chorioangioma of the placenta. Gynaecol Obstet Invest 1989;28:108‑110.
- Marchetti
AA. A consideration of certain types of benign tumors of the placenta. Surg Gynecol Obstet 1939;68:733‑743.
- Wallenburg
HCS. Chorioangioma of the placenta. Obstet Gynecol Surv 1971;26:411‑24.
- Resnick
L. Chorioangioma with report of a case
associated with oligohydramnios.
- Froehlich LA, Fujikura T,
Fisher P. Chorioangiomas and their clinical
implications. Obstet Gynecol
1971;37:51‑59.
- Heggtveit
HA, DeCarvalho R, Nuyens
AJ. Chorioangioma and toxemia of pregnancy. Am J
Obstet Gynecol 1965;91:291‑292.
- King PA,
Lopes A, Tang MY, et al. Theca lutein ovarian
cysts associated with placental chorioangioma.
Br J Obstet Gynaecol
1991;98:322‑323.
- Reiner
L, Fries E. Chorioangioma associated with arterio‑venous aneurysm. Am J Obstet Gynecol 1965;93:58‑64.
- Achiron
R, Shaia M, Schimmel
M, Glasser J. Choriangioma
with hydrops in twins. The Fetus 1992;2 (3): 7622 1‑3.
- Hadi
HA, Finley J, Strickland D. Chorioangioma:
prenatal diagnosis and clinical significance. Am J Perinatol
10 (2): 146‑9, 1993.
- Jones CEM, Rivers RPA, Taghizadeh A. Disseminated intra‑vascular
coagulation and fetal hydrops in a newborn
infant in association with a chorioangioma of
placenta. Pediatrics 1972;50: 901‑907.
- Franca‑Martins AMC,
- Sims DG, Barron SL, Wadehara V, et al. Massive chronic feto‑maternal
bleeding associated with choriangiomas. Acta Pediatr Scand 1976;65:271‑273.
- Wurster
DE, Hoetnagel D, Bernischke
K, et al. Placental chorangiomata and mental
deficiency in a child with 2/15translocations: 46,XX, t(2q‑;15 q+). Cytogenetics 1969;8:389‑399.
- Verloes
A, Schaaps JP, Herens
C, et al. Prenatal diagnosis of cystic hygroma
and chorioangioma in the Wolf‑Hirschhorn syndrome. Prenat Diagn 1991;11:129‑132.
- Quintero
RA, Reich H, Romero R, Johnson MP, Goncalves L,
Evans MI. In utero endoscopic
devascularization of a large chorioangioma.
Ultrasound Obstet Gynecol
1996; 8: 48-52.
- Stiller
AG, Skafish PR. Placental chorioangioma:
a rare cause of fetomaternal transfusion with
maternal hemolysis and fetal distress. Obstet Gynecol
1986; 67: 296-298.
- Sepulveda
W, Aviles G, Carstens E, Corral E, Perez N.
Prenatal diagnosis of solid placental masses: the value of color flow
imaging. Ultrasound Obstet Gynecol 2000; 16: 554-558.
- Zalel Y, Weisz B, Gamzu R, Schiff E, Shalmon B, Achiron R. Chorioangiomas of the placenta: sonographic
and Doppler flow characteristics. J Ultrasound Med 2002; 21: 909-913.
- Prapas N, Liang RI, Hunter D, Copel
JA, Lu LC, Pazkash V, Mari G. Color Doppler
imaging of placental masses: differential diagnosis and fetal outcome. Ultrasound
Obstet Gynecol
2000; 16: 559-563.
- Shih
JC, Cheng WF, Shyu MK, Lee CN, Hsieh FJ. Power
Doppler evidence of placenta accreta appearing
in the first trimester. Ultrasound Obstet Gynecol 2002; 19: 623-625.
- Chou
MM, Tseng JJ, Ho ESC. The application of three-dimensional color power
Doppler ultrasound in the depiction of abnormal uteroplacental
angioarchitecture in placenta previa percreta. Ultrasound
Obstet Gynecol
2002; 19: 625-627.
- Jauniaux
E, Ogle R. Color Doppler imaging in the diagnosis and management of chorioangiomas. Ultrasound Obstet
Gynecol 2000; 15: 463-467.
- Chazotte
C, Girz B, Koenigsberg
M, Cohen WR. Spontaneous infarction of placenta chorioangioma
and associated regression of hydrops fetalis. Am J Obstet Gynecol 1990; 163: 1180-1181.
- Hsieh
CC, Soong YK. Infarction of placental chorioangioma and associated regression of hydrops fetalis. Am J Obstet Gynecol 1992; 166: 1306.