|
PLACENTA ACCRETA |
Placenta accreta is abnormal attachment of the placenta to the uterine wall.
Pathologically there is a diminished or absent decidua basalis.
ETIOLOGY |
ULTRASOUND |
In the first trimester:
The usual location of a normal early gestation is in the fundus or very occasionally in the lower uterine segment. The sac is surrounded by thick myometrium on all sides.
- Placenta accreta (and percreta) does occur in the first trimester. It is usually discovered during dilatation and curettage when massive bleeding occurs due to placental invasion of the myometrium by placenta (1-9).
- Individuals who are at risk for placenta accreta at term are also at risk for placenta accreta in the first trimester, i.e. scarring of the uterus by surgical incision is a risk factor in the first trimester as well as later in pregnancy.
- It may present as a low-lying sac that appears to be attached to the anterior wall of the uterus or uterine scar. The myometrium was thin in the area of the scar to which the sac was attached.
· As early as 16 weeks irregular vascular sinuses appear, which have turbulent flow within them.
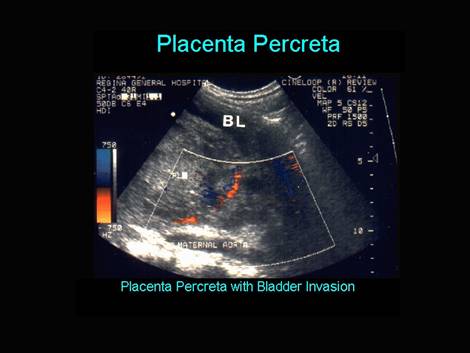
· The bladder wall may appear interrupted or have small bulges of the placenta into the bladder space.
· Absence of the normal echolucent space between the placenta and myometrium is not a reliable sign by itself, since this space may be absent in normal patients with an anterior placenta.
· Color Doppler will show that some of the placental sinuses traverse the uterine wall.
· Magnetic resonance imaging has not yet been shown to aid in the diagnosis, but in the future, with improvement of resolution and shortened sequences, it should be particularly useful in identifying the patients that have placenta percreta
In the second and third trimesters:
- The area of interest is the retroplacental hypoechoic space.
- Normal = 1cm (seen after 18 weeks) (10).
- Placenta accreta - absence or thinning of this hypoechoic zone especially in a patient with a low lying placenta or placenta previa.
- Ultrasound criteria for placenta accreta (11).
1. Thinning (<1 mm) or absence of the hypoechoic myometrial zone in the anterior lower uterine segment between the placenta and the echodense boundary zone representing the uterine serosa and posterior bladder wall.
2. Thinning, irregularity, or focal disruption of the linear, hyperechoic uterine serosa / bladder wall complex.
3. The presence of focal mass-like elevations or extensions of tissue, with the same echogenicity as placenta, beyond the uterine serosa.
4. The presence of lacunar vascular spaces in the placenta. Although the cause of placental lacunae is unknown, many authors have found them to be predictive of placenta accrete (12-15). Visualization of lacunae had the highest sensitivity (79%) in the 15-20-week range and a sensitivity of 93% in the 15-40-week gestational age time frame. Twickler et al (15) made the additional point that not only did these intraplacental sonolucencies predict all cases of accreta (with three false positives) but also that the lacunae did not need to be near the area of invasion. Finberg and Williams found that the likelihood of placenta accreta increased with the number of lacunae (14).
The lacunae:
· have a moth-eaten appearance to the placenta.
· usually, but not always, have turbulent flow within them,
· irregular, often more linear rather than rounded and smooth bordered.
· do not have the highly echogenic border that standard venous sinuses have.
· Tornado-shaped flow of venous, arterial or mixed blood is typical.
· These sinuses have been seen as early as 9 weeks' gestation (15). Not all large sinuses or vessels are associated with placenta accreta.
· Large sinuses in patients who did not have placenta accreta can be occasionally seen (these sinuses are smooth in contour and quite round).
Bladder border
· The border between the bladder and myometrium is normally highly echogenic and smooth.
· In the case of placenta accreta, interruptions or bulging can occur and Finberg and Williams (14) found that this is a specific sign, but not a sensitive one, i.e. interruptions or bulging are not present in every patient with placenta accreta. However, this can be a problem in that patients who have had a Cesarean section often develop increased vascularity in the space between the myometrium and the bladder, probably because the bladder flap is retracted before the incision is made into the uterus and because this area is exposed to blood products. Therefore, it would be important to differentiate between bulging due just to enlarged or increased number of vessels and actual growth through the myometrium.
· Bulging is somewhat non-specific for placenta percreta involving the bladder and does not always predict these cases. In the three cases in our series in which this sign was present, two had a placenta percreta. Kirkinen et al. noted a bulging of the placenta into the bladder in two of their cases of placenta accreta but there was no growth into the bladder (16). Thus, it appears that bulging of the bladder wall may indicate accreta but does not diagnose percreta. Care must be taken to examine the bladder wall with the ultrasound transducer at 90° so that it is clearly seen.
Myometrial thickness
· Twickler et al. measured the thickness of the lower uterine segment in women who had had a previous Cesarean section and had a low-lying anterior placenta or placenta previa by measuring between the bladder wall and the retroplacental vessels, as seen by color Doppler. All patients later proven to have placenta accreta had a myometrium of less than 1 mm (15), which was as predictive of accreta as lacunae. .
Loss of the clear space
· The usual dark line between the myometrium and the placenta is thought to represent the decidua basalis. Since the decidua basalis is absent in placenta accreta, it has been suggested that the absence of this line suggests placenta accreta. This line may be absent in many normal patients with anterior placentas (17).
Doppler
· Lerner et al. found that turbulent blood flow extending from the placenta into surrounding tissues was very sensitive and correctly identified all patients with accreta. This finding was not present in any of the patients without accrete (18).
· Levine et al., in a blinded study, found that power Doppler did not improve the diagnosis of placenta accrete (19).
· Chou et al. used Doppler in the third trimester and thought that it was reliable. However, on close examination gray-scale images appeared to be as effective and color Doppler could not distinguish accreta from increta (20).
|
|
|||||||
|
Normal retroplacental hypoechoic zone Loss of the retroplacental hypoechoic zone |
Loss of the retroplacental hypoechoic zone
which most likely corresponds to the decidua basalis, myometrium, and dilated
venous channels (7,8)
Progressive thinning of the retroplacental
hypoechoic zone on serial examinations |
||||||
|
Normal hyperechogenic boundary line Loss of the hyperechogenic boundary line
between the uterine serosa and wall of the bladder |
|
||||||
|
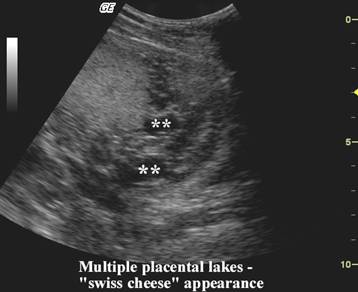
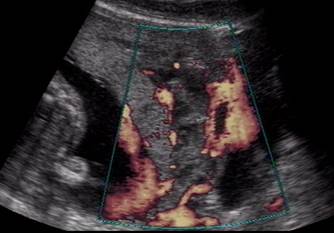
Multiple placental lakes |
Multiple placental lakes that may represent
dilated vessels extending from the placenta through the myometrium—the
so-called "Swiss cheese" appearance of the placenta (9) |
||||||
|
Thinning of the
uterine serosa-bladder wall complex (percreta) |
|
||||||
|
Focal mass-like
elevation of tissue with the same echogenicity as the placenta beyond the
uterine serosa (percreta) (1) |
|
||||||
|
Elevation of
tissue beyond the uterine serosa (percreta) |
|
||||||





|
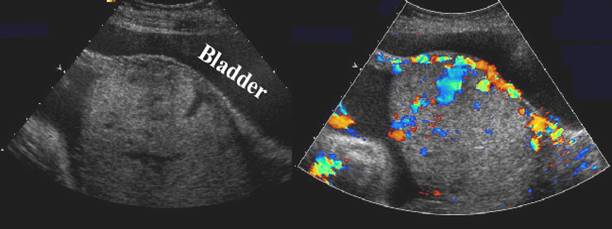
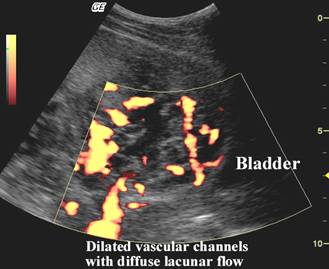
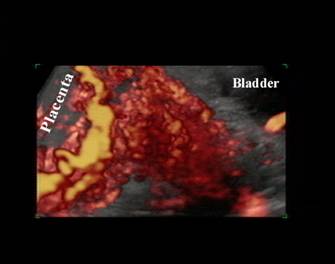
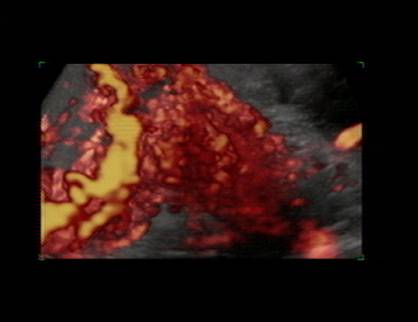
Color and Power
Doppler Imaging Detection rates of placenta accreta with color
and power doppler imaging, especially anterior placenta accreta, have been
high, because it can detect with a high level of confidence abnormal
uteroplacental hypervascularity caused by the angiogenesis of placental
invasion. |
||
|
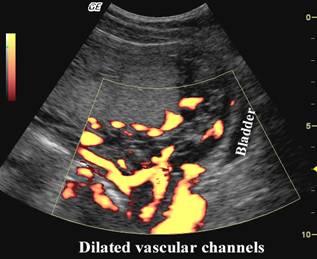
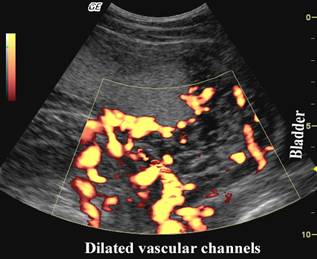
Dilated vascular
channels with diffuse lacunar flow |
A diffuse lacunar flow
pattern from dilated vascular channels scattered throughout the whole
placenta and the surrounding myometrial or cervical tissues. High velocity
pulsatile venous-type flow can be found in the sonolucent vascular spaces. A
finding of this nature has been associated with a higher level of maternal
morbidity and mortality. |
|
|
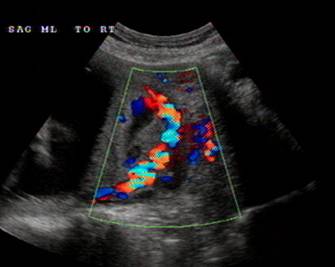
Irregular
vascular lakes with focal lacunar flow |
A focal lacunar flow
pattern showing irregular sonolucent vascular lakes with turbulent lacunar
flow distributed regionally or focally within the intraparenchymal placental
area. |
|
|
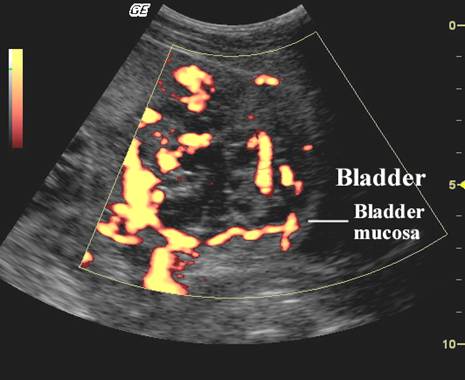
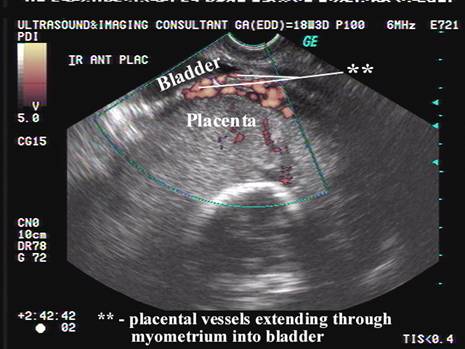
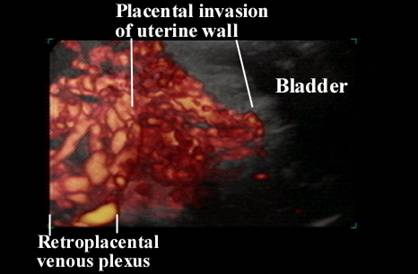
Hypervascularity
linking placenta to bladder |
Interface
hypervascularity with abnormal blood vessels linking the placenta to the
bladder |
|
|
Dilated vascular channels |
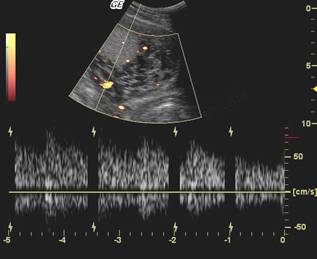
Markedly dilated
peripheral subplacental vascular channels with pulsatile venous-type flow
over the uterine cervix. |
|
|
Poor vascularity at sites of loss of hypoechoic zone. |
Absence of
subplacental vascular signals in the areas lacking a peripheral hypoechoic
zone. |
|
|
3D Ultrasound |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|






COMPLICATIONS |
- Massive vaginal bleeding (intra- and postpartum).
- Uterine wall rupture.
- Invasion of adjacent structures.
- Uterine infection.
- Uterine inversion due to attempted manual removal of the placenta (22-24).
MORTALITY RATE |
- 25% infant mortality rate (23,24).
- 10% maternal mortality (23,24).
REFERENCES |
- Miller DA, Chollet JA, Goodwin TM. Clinical risk factors for placenta previa- placenta accreta. Am J Obstet Gynecol 1997; 177: 210-214.
- Harden MA, Walters MD, Valente PT. Postabortal hemorrhage due to placenta increta: a case report. Obstet Gynecol 1990; 75: 523-526.
- Woolcott RJ, Nicholl M, Gibson JS. A case of placenta percreta presenting in the first trimester of pregnancy. Aust N Z J Obstet Gynaecol 1987; 27: 258-260.
- Ecker JL, Sorem KA, Soodak L, Roberts DJ, Safon LE, Osathanondh R. Placenta increta complicating a first-trimester abortion. A case report. J Reprod Med 1992; 37: 893-895.
- Walter
AJ, McCullough AE, Patel MD,
- Gherman RB, McBrayer S, Tichenor J, Wing DA. Placenta increta complicating first-trimester D&C. Obstet Gynecol 1999; 93: 845.
- Chanrachakul B, Hamontri S, Leopairut J, Herabutya Y. Placenta increta complicating the first trimester abortion. Acta Obstet Gynecol Scand 2001; 80: 467-468.
- Höpker M, Fleckenstein G, Heyl W, Sattler B, Emons G. Placenta percreta in week 10 of pregnancy with consecutive hysterectomy: case report. Hum Reprod 2002; 17: 817-820.
- Nelson LH. Ultrasonography of the placenta - A review. Laurel MD, AIUM, 1994
- Benirschke K, Driscoll SG.
Unusual shapes of the placenta. In: Benirschke K, Driscill SG: The
pathology of the human placenta.
- Kerr de Mendoncaq L. Sonographic diagnosis of placenta accreta, presentation of six cases. J Ultrasound Med 1988; 7: 211-215.
- Hoffman-Tretin JC, Koenigsberg M, Rabin A, Anyaegbunam A. Placenta accreta. Additional sonographic observations. J Ultrasound Med 1992; 11: 29-34.
- Finberg HJ, Williams JW. Placenta accreta: prospective sonographic diagnosis in patients with placenta previa and prior cesarean section. J Ultrasound Med 1992; 11: 333-343.
- Twickler DM, Lucas MJ, Balis AB, Santos-Ramos R, Martin L, Malone S, Rogers B. Color flow mapping for myometrial invasion in women with a prior cesarean delivery. J Matern Fetal Med 2000; 9: 330-335.
- Kirkinen P, Helin-Martikainen H, Vanninen R, Partanen K. Placenta accreta: imaging by gray-scale and contrast-enhanced color Doppler sonography and magnetic resonance imaging. J Clin Ultrasound 1998; 26: 90-94
- McGahan JP, Phillips HE, Reid MH. The anechoic retroplacental area: a pitfall in diagnosis of placental-endometrial abnormalities during pregnancy. Radiology 1980; 134: 475-478.
- Lerner JP, Deane S, Timor-Tritsch IE. Characterization of placenta accreta using transvaginal sonography and color Doppler imaging. Ultrasound Obstet Gynecol 1995; 5: 198-201.
- Levine D, Hulka CA, Ludmir J, Li W, Edelman RR. Placenta accreta: evaluation with color Doppler US, power Doppler US, and MR imaging. Radiology 1997; 205: 773-776.
- Chou MM, Tseng JJ, Ho ES. The application of three-dimensional color power Doppler ultrasound in the depiction of abnormal uteroplacental angioarchitecture in placenta previa percreta. Ultrasound Obstet Gynecol 2002; 19: 625-627.
- Breen JL, Neubecker R,
- Fox H. Placenta accreta.
In: Fox H: Pathology of the placenta.
- Aho AJ,
- Kim JA, Narra VR. Magnetic resonance imaging with true fast imaging with steady-state precession and half-Fourier acquisition single-shot turbo spin-echo sequences in cases of suspected placenta accreta. Acta Radiol 2004; 45: 692-698.
- Lam G, Kuller J, McMahon M. Use of magnetic resonance imaging and ultrasound in the antenatal diagnosis of placenta accreta. J Soc Gynecol Investig 2002; 9: 37-40. Links
- Ito T, Katagiri C, Ikeno S, Takahashi H, Nagata N, Terakawa N. Placenta previa increta penetrating the entire thickness of the uterine myometrium: ultrasonographic and magnetic resonance imaging findings. J Obstet Gynaecol Res 1999; 25: 303-307