|
ULTRASOUND OF SINGLE
UMBILICAL ARTERY (1-14) |
The sonographic diagnosis of SUA can be made as early as 12 weeks gestation, although the highest rates of detection are at 17 to 35 weeks (12).
Evaluation of the umbilical arteries can be done by looking at a free portion of the cord, either longitudinally or in cross-section, or by using color Doppler in the area of the fetal abdominal cord insertion site to identify the umbilical arteries as they course on either side of the fetal bladder. It is by the latter method that the side of the missing umbilical artery can be determined.
Some authors have suggested that visualization of the vessels around the fetal bladder may not be as accurate as looking at a free loop of cord (12,13), primarily because it seems to increase the false-positive rate.
Using a transverse view of a free loop of the umbilical cord to make the diagnosis of SUA, transabdominal sonography was reported in one series to have an 85% sensitivity, a 99.7% specificity, an 85% positive predictive value, and a 99.7% negative predictive value for the detection of a two-vessel cord (12). The false-positive rate in this series was only 0.03%; in another series that used both a cross-sectional image of the umbilical cord and visualization of the two vessels coursing around the bladder, the false-positive rate was much higher (14%) (12-14).
|
|
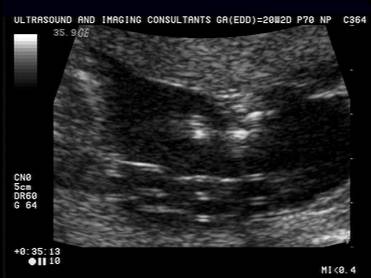
GRAY-SCALE IMAGES |
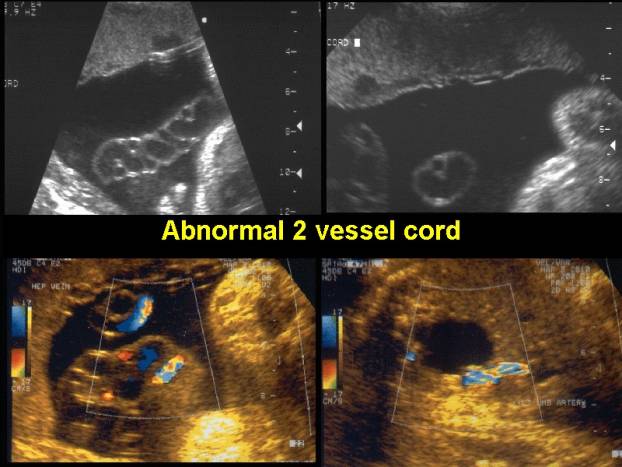
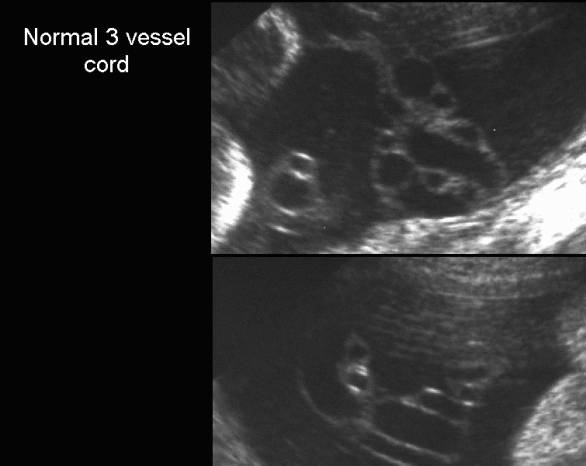
- Absent "Mickey Mouse" appearance on transverse images.
|
|
- Loss of the normal helical braided appearance on sagittal sections.
- There is an increased number of absent and right coiling associated with single umbilical artery.
- There is frequently a decreased amount of Whartons jelly (lean cord).
|
Single umbilical artery.
|
|
|
|
|
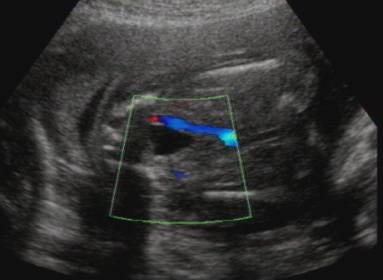
Single umbilical artery
|
|
|
|
|

- Either the left or right umbilical artery may be absent (absence of the left artery appears to be more frequent).
- A two and three vessel cord may be demonstrated at different locations within the same umbilical cord.
- The presence of a normal and small umbilical artery suggests atrophy or atresia of a previously normal artery.
|
Two and three vessel cord in the same fetus at slightly different
levels. |
|
|
|
|
|
|
|




COLOR DOPPLER IMAGING OF THE CORD |
- Allows for better and earlier diagnosis of cord anomalies (1,2).
- It helps to detect discrepancy in size in cases of oligohydramnios, twins or when multiple loop of cord makes size evaluation difficult.
- It can confirm the presence of flow within a hypoplastic artery (3).
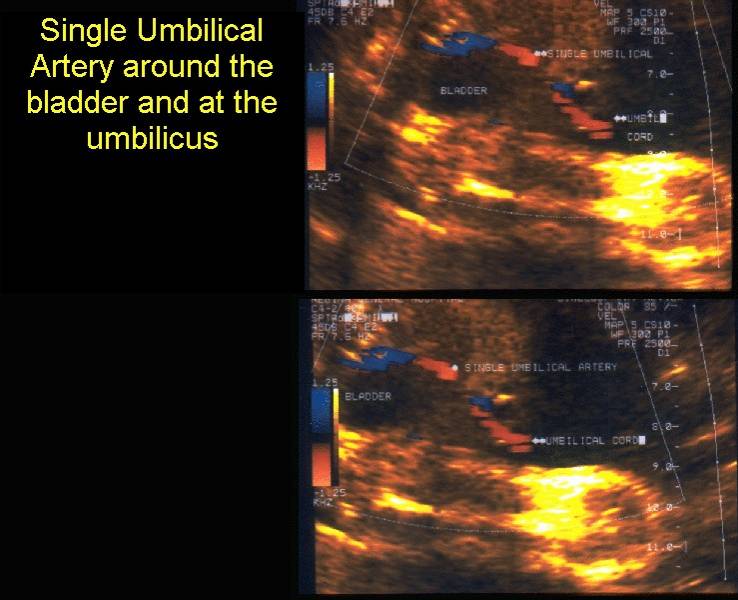
COLOR DOPPLER IMAGING OF THE FETAL PELVIS |
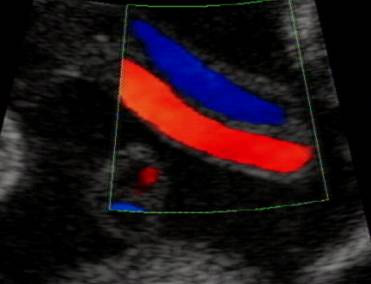
- The intrafetal portion of the umbilical arteries is usually much easier to visualize, as they are not distorted by the tortuosity and spiraling of the umbilical cord.
- Normally the vessels can be traced from their origin at the fetal iliac arteries, around the urinary bladder until they converge at the umbilicus.
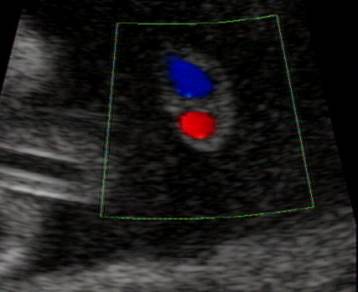
Single umbilical artery around the bladder |
Normal – two umbilical arteries around the bladder |
|
|
|
|
|
|

|
Video clip of single umbilical artery
–differentiation from the common iliac artery |
- The absence of one umbilical artery can easily be recognized especially when oligohydramnios or premature rupture of membranes are present.
PULSED DOPPLER |
Doppler flow indices in normal and small for gestational age fetuses with SUA are not significantly different from normal fetuses (4). This has been attributed to compensatory arterial dilatation in the single umbilical artery, which acts to prevent growth retardation.
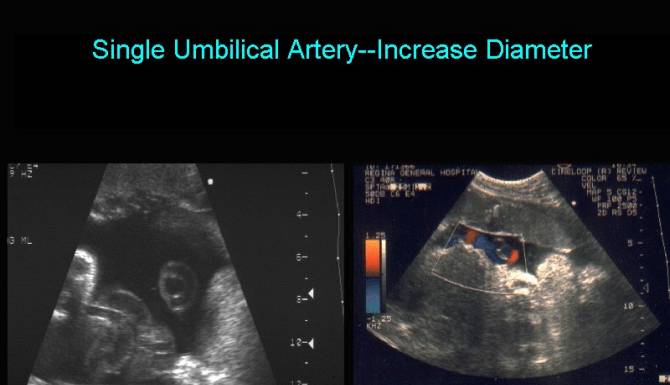
DIAMETER OF THE UMBILICAL CORD |
- Sepulveda and co-workers (5) - fetuses with SUA, the diameter of the artery was larger than 50% of the vein (ratio of umbilical vein to artery (2).
- Persutte and Lenke (6) - a transverse umbilical arterial diameter of >4mm was predictive of a SUA between 20-36 weeks gestation.
The above studies assume a compensatory increase in the size of the
remaining umbilical artery. Brohnshtein and Zimmer
(7) did not confirm these observations. The differences may be due to the
technical limitations that are inherent when accurately trying to measure cord
vessels (6):
- Limits of resolution (0.5-1.5mm axially and poorer lateral resolution).
- Intra observer variability (at least ±0.5mm).
- Variable diameter of the vessels along the cord.
- Diameter of both arteries is not always identical (8-10).
- Transverse section of the cord is not always circular.
De Catte (4) demonstrates that measurements taken when the arterial wall lining on both sides is brightly echogenic means the ultrasound beam are perpendicular to the arterial wall. If the vessel was truly circular only a small echogenic spot should be present. A large echogenic line means the vessel is elliptical at some points.
|
|
- Effect of fetal behavior.
Measurements obtained at
different states of fetal activity may demonstrate differences in blood flow
and vessel diameter.
Gill and colleagues (11) - 10% variation in umbilical vein diameter and 20%
difference in blood flow on repeated measurements.
It is important to distinguish between SUA and fusion of the two umbilical arteries. Umbilical artery fusion may occur completely or intermittently along the length of the umbilical cord (16). Fusion of the two arteries may be mistaken for SUA if multiple portions of the cord are not examined. The frequency of fusion of the two umbilical arteries was found to be 3.1% in one study of placentas from 702 consecutive deliveries (17). The low frequency of SUA in this series (0.2%) may reflect the true incidence of SUA in the general population when fusion of the two umbilical arteries has been excluded. It is important to distinguish between fusion of the two umbilical arteries and SUA whenever possible, because there is no evidence that fusion of the two umbilical arteries is associated with adverse perinatal outcomes (17,18). If both two- and three-vessel cords are identified, the patient should be considered to have a normal three-vessel umbilical cord (19). Like SUA, fusion of the two umbilical arteries has been associated with increased rates of marginal (18.1%) and velamentous (4.5%) cord insertions (17) as compared with singletons.
Sonographic Approach:
Because the finding of SUA carries with it a substantially increased risk of congenital abnormalities and aneuploidy, the finding of SUA on a second-trimester ultrasound should prompt an immediate detailed ultrasound examination to rule out any associated abnormalities. Referral to an experienced center should be done whenever necessary.
Fetal echocardiography should be obtained:
· In one series, 5% of fetuses referred for fetal echo with presumed isolated SUA had abnormal findings (15).
· In another series, however, fetal echo did not add any diagnostic information in fetuses with SUA when the normal four-chamber and outflow tract views of the heart had been obtained satisfactorily (14).
Invasive testing for chromosome analysis should be recommended if any associated abnormalities are identified on sonogram, including structural anomalies, oligohydramnios, polyhydramnios, and IUGR.
In the absence of associated anomalies, invasive testing is not warranted, because there is no increased risk of aneuploidy.
Patients should be counseled, however, that even when SUA is apparently isolated 7% of fetuses in one series had structural anomalies diagnosed postnatally, which if diagnosed prenatally would have resulted in a recommendation for invasive testing (20).
Serial growth scans are warranted, because SUA has been associated with increased rates of IUGR. Antenatal testing is recommended in the setting of IUGR or oligohydramnios. Doppler studies should also be used to assess the status of an IUGR fetus. Despite there being only one umbilical artery, it has been shown that longitudinal changes in Doppler flow indices in normal and small-for-gestational-age fetuses with SUA have comparable reference ranges to fetuses with three-vessel cords (4). A large prospective series of umbilical artery Doppler velocimetry in pregnancies with a SUA found that abnormal Doppler findings were associated significantly with IUGR, presence of complex malformations, aneuploidy, preterm delivery, and perinatal mortality. Conversely, normal umbilical artery Doppler indicates a relatively good prognosis, in particular a low-risk of fetal aneuploidy or perinatal mortality (21). Unlike umbilical artery blood flow, the ductus venosus blood flow pattern seems to be different in SUA fetuses when compared with that of fetuses with three-vessel cords (22). Future studies are needed to evaluate individual Doppler parameters in the fetus with SUA before they can be used routinely in these fetuses.
REFERENCES |
- Nyberg DA, Mahony BS, Luthy D, Kapur R. Single umbilical artery: prenatal detection of concurrent anomalies. J Ultrasound Med 1991;10:247.
- Jauniaux W, Campbell S, Vyas S. The use of color doppler imaging for prenatal diagnosis of umbilical cord abnormalities: report of three cases. Am J Obstet Gynecol 1989;161:1195.
- Sepulveda W, Flack NJ, Bower S, Fisk NM. The value of color doppler ultrasound in the prenatal diagnosis of hypoplastic umbilical artery. Ultrasound Obstet Gynecol 1994;4:143-146.
- De Catte L, Burrini D, Mares C, Waterschoot T. Single umbilical artery: analysis of doppler flow indices and arterial diameters in normal and small-for-gestational age fetuses. Ultrasound Obstet Gynecol 1996;8:27-30.
- Sepulveda W, Peek MJ, Hassan J, Hollingsworth J. Umbilical vein to artery ratio in fetuses with single umbilical artery. Ultrasound Obstet Gynecol 1996;8:23-26.
- Persutte WH, Lenke RR. Transverse umbilical arterial diameter: technique for the prenatal diagnosis of single umbilical artery. J Ultrasound Med 1994;13:763-766.
- Bronshtein M, Zimmer EZ. Are measurements of the umbilical vessels a reliable method in diagnosing single umbilical artery? Ultrasound Obstet Gynecol 1996;8:5-7.
- Trudinger BJ, Cook CM. Different umbilical artery flow velocity waveforms in one patient. Obstet Gynecol 1988;71:1019-1021.
- Harper MA, Murnagham GA. Discordant umbilical artery flow velocity waveforms and pregnancy outcome. Br J Obstet Gynaecol 1989;96:1449-1452.
- Dolkart LA, Reimers FT, Kuonen CA. Discordant umbilical arteries: ultrasonic and doppler analysis. Obstet Gynecol 1992;79:59-63.
- Gill RW, Trudinger BJ, Garret WJ et.al.
Fetal umbilical venous flow measured in utero by
pulsed doppler and B-mode ultrasound. Am J Obstet Gynecol 1981;139:720-725.
- Hill
LM, Wibner D, Gonzales P, Chenevey
P. Validity of transabdominal sonography in detection of a two-vessel umbilical
cord. Obstet Gynecol
2001;98:837-42.
- Bornemeier S, Carpinito LA,
Winter TC. Sonographic evaluation of the two
vessel umbilical cord: a comparison between umbilical arteries adjacent to
the bladder and cross-sections of the umbilical cord. J Diagn Med Sonogr 1996;12:260-5.
- Sepulveda
W, Dezerega V, Carstens
E, Gutierrez J. Fused umbilical arteries: prenatal sonographic
diagnosis and clinical significance. J Ultrasound Med 2001;20:59-62.
- Fujikura
T. Fused umbilical arteries near placental cord insertion. Am J Obstet Gynecol 2003;188:765-7.
- Heifetz
SA. Single umbilical artery: a statistical analysis of 237 autopsy cases
and review of the literature. Perspect Pediatr Pathos 1984;8:345-87.
- Hill
LM, Wibner D, Gonzales P, Chenevey
P. Validity of transabdominal sonography in detection of a two-vessel umbilical
cord. Obstet Gynecol
2001;98:837-42.
- Chow
JS, Benson CB, Doubilet PM. Frequency and nature
of structural anomalies in fetuses with single umbilical arteries. J Ultrasound
Med 1998;17:765-8.
- Ulm
B, Ulm MR, Deutinger
J, Bernaschek G. Umbilical artery Doppler velocimetry in fetuses with a single umbilical artery.
Obstet Gynecol 1997;90:205-9.
- Raio
L, Ghezzi F, Di Naro E, Franchi M, Bruhwiler H, Luscher KP.
Prenatal assessment of Wharton's jelly in umbilical cords with single
artery. Ultrasound Obstet Gynecol
1999;14:42-6.