ULTRASOUND IN OMPHALOCELE |
The diagnosis is usually made after the 12th week of gestation once the
normal physiological hernia has resolved (bowel containing omphaloceles). Liver
herniation is not a feature of normal physiological bowel herniation, and
therefore eviscerated liver permits diagnosis of omphalocele at any age. Liver
containing omphaloceles are more homogeneous and less echogenic than normal physiological herniation (1,2).
First trimester diagnosis of liver containing omphaloceles have been made (1,2):
·
Omphalocele at 13 weeks as an echogenic tumor at
the umbilicus; the fetus was subsequently found to have trisomy 18 (4).
·
Omphalocele containing liver at 10 weeks, but
retrospective examinations of the sonograms obtained at 6–9 weeks did not
reveal any abnormality; the diagnosis was confirmed after delivery (4).
·
Pagliano et al. (6) reported the diagnosis
of omphalocele containing liver and bowel in a 10-week fetus.
·
Heydanus et al. (7) reported the diagnosis
of omphalocele in three fetuses at 12–14 weeks; in one there was an
associated ectopia cordis and hydrops and the pregnancy was terminated, in the
second there was an associated two-vessel cord and intrauterine death occurred
and, in the third with isolated exomphalos, there was an infant death.
·
van Zalen-Sprock et al. (8) reported the
findings of 14 cases with omphalocele diagnosed at 11–14 weeks of
gestation. In eight cases, there was increased nuchal translucency thickness
(3.5–10 mm) and seven of these had chromosomal abnormalities, mainly
trisomy 18. The contents of the omphalocele were bowel only in the
chromosomally abnormal group and liver as well as bowel in those with a normal
karyotype. In the chromosomally normal group, there were four with other
defects, such as tetralogy of Fallot and Meckel–Gruber syndrome; only
three infants were liveborn.
·
An ultrasound screening study of 622 high-risk
pregnancies at 10–13 weeks correctly diagnosed the two cases of
omphalocele (9).
·
In two other screening studies of low-risk
patients, involving 1632 pregnancies at 12–14 weeks (10) and
1473 pregnancies at 10–14 weeks (11), respectively, there were four cases
of Omphalocele (two in each) and they were all diagnosed in the first-trimester
scan.
·
In a screening study for chromosomal abnormalities
by assessment of fetal nuchal translucency thickness at 10–14 weeks of
gestation, there were 15 726 pregnancies with a minimum gestation of 11 weeks
and 4 days and, in this group, there were 18 cases of omphalocele. In seven
cases, the karyotype was normal, in nine there was trisomy 18, in one trisomy
13 and in one triploidy. The prevalence of omphalocele in fetuses with trisomy
18 was 23%, in those with trisomy 13 it was 9%, in those with triploidy it was
13% and in those with no evidence of these chromosomal defects it was 0.045%.
This study demonstrated that both the prevalence of omphalocele and the
associated risk for chromosomal defects increase with maternal age and decrease
with gestational age (12).
ULTRASOUND
|
- Midline ventral abdominal wall defect (2.5-5 cm).
- Umbilical cord inserts into the apex of the defect.
- Widening of the cord where it joins the abdominal skin.
- Herniation of abdominal viscera at the base of the umbilical cord.
- Intracorporeal liver. Bowel containing omphaloceles have a strong association with an abnormal karyotype (2).
- Extracorporeal liver. Lower frequency of chromosomal anomalies (2)
- An omphalocele membrane is almost always present and is composed of two layers (the inner peritoneal membrane and outer amnion).
- Ascites within the sac is commonly present (3).
- Hypoechoic Wharton's jelly can often be found between the membranes.
- Polyhydramnios.
- Occasionally oligohydramnios.
Liver containing omphalocele in the first trimester |
|
Liver containing omphalocele in the third trimester
|
|
|
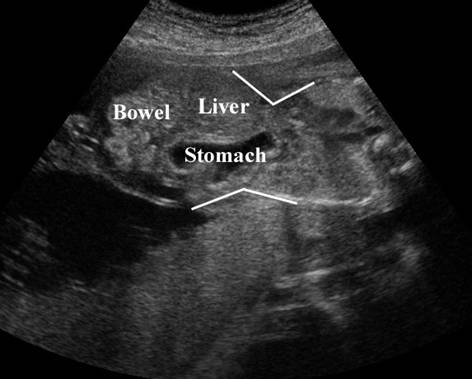
Liver and bowel containing omphalocele in the second
trimester |
|
Bowel containing omphalocele in the second trimester |
|
|
|
|
|
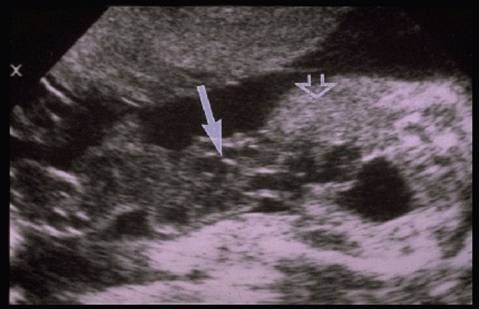
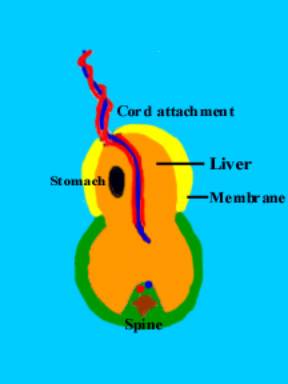
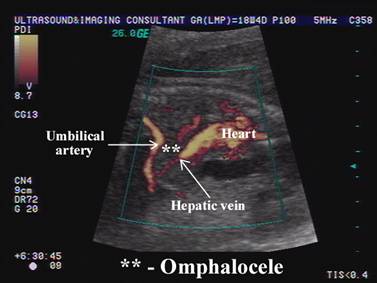
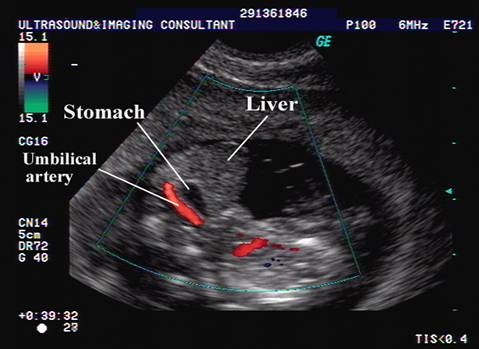
Omphalocele containing
liver, bowel and stomach |
|
|
|
|
|
|
|
|
|
|
Cord insertion |
|
|
|
|
|
|
|
|
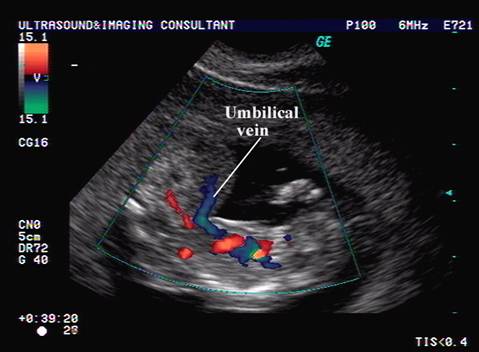
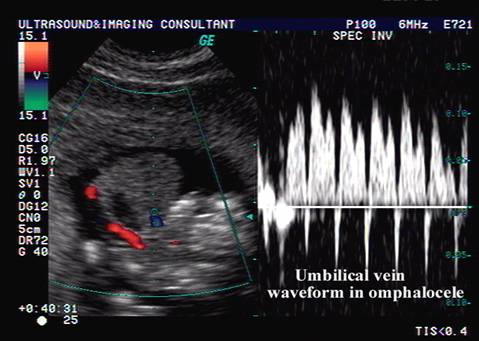
Cord doppler |
|






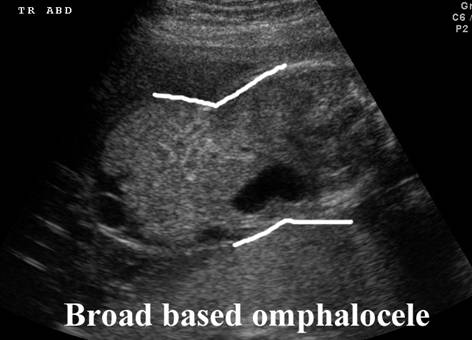



- Broad - based omphalocele – there is a wide angle between the omphalocele sac wall and the abdominal wall. When the angle is obtuse (greater than 90 degrees), the defect may go unnoticed, especially if the omphalocele contains liver. These type of omphaloceles are best detected on midline sagittal scans.
|
Narrow based
Omphalocele Note
the acute angle between the omphalocele and fetal abdominal wall |
Broad based
Omphalocele Note the obtuse angle between
the omphalocele and fetal abdominal wall |
|
|
|
|
|
|



REFERENCES |
- Brown Dl, Emerson DS, Shulman LP et.al. Sonographic diagnosis of omphalocele during 10th week of gestation. AJR 1989;153:825-826.
- Curtis JA, Watson L. Sonographic diagnosis of omphalocele in the first trimester of fetal gestation. J Ultrasound Med 1988;7:97-100.
- Emanuel PG, Garcia GI, Angtuaco TL. Prenatal detection of anterior abdominal wall defects with US. Radiographics 1995;15:517-530.
- Schmidt W, Kubli F. Early diagnosis of severe congenital malformations by ultrasonography. J Perinat Med 1982;10:233–41
- Brown DL, Emerson DS, Shulman LP, Carson SA. Sonographic diagnosis of omphalocele during the 10th week of gestation. Am J Radiol 1989;153:825–6
- Pagliano M, Mossetti M, Ragno P. Echographic diagnosis of omphalocele in the first trimester of pregnancy. J Clin Ultrasound 1990;18:658–60
- Heydanus R, Raats AM, Tibboel D et.al. Prenatal diagnosis of fetal abdominal wall defects: a retrospective analysis of 44 cases. Prenat Diagn 1996;16:411–17
- van Zalen-Sprock RM, van Vugt JMG, van Geijn HP. First-trimester sonography of physiological midgut herniation and early diagnosis of omphalocele. Prenat Diagn 1997;17:511–18
- Goldstein RB, Filly RA, Callen PW. Sonography of anencephaly: pitfalls in early diagnosis. J Clin Ultrasound 1989;17:397–402
- Economides DL, Braithwaite JM. First trimester ultrasonographic diagnosis of fetal structural abnormalities in a low risk population. Br J Obstet Gynaecol 1998;105:53–7
- Timor-Tritsch IE, Monteagudo
A,
- Kushnir O, Izquierdo L, Vigil D, Curet LB. Early transvaginal diagnosis of gastroschisis. J Clin Ultrasound 1990;18:194–7