THE THICK UMBILICAL CORDABNORMALITIES OF CORD
MATRIX |
|
1.
Diabetes mellitus. |
|
|
|
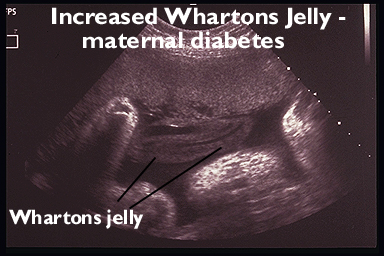
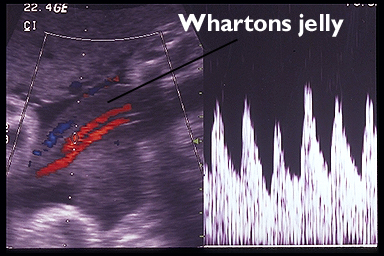
- Weissmann and Jakobi (1) reported that the sonographic umbilical cord area and the WJA of diabetic fetuses, even if not macrosomic, are significantly greater than those in healthy fetuses. Importantly, sonographic modifications of the umbilical cord of diabetic fetuses have been noted as early as 24 weeks of gestation.
- Raio et al. (2)
reported that fetuses with a sonographically lean umbilical cord present
an increased risk of growth abnormalities, distress in labor and
oligohydramnios.
· Fetuses with Turner syndrome might have a wider than normal umbilical cord.
1. The most plausible mechanism to explain the cytic hygromata that is present in fetuses with Turner syndrome is lymphatic vessel hypoplasia in the upper dermis (3).
2. This does not explain the increased umbilical cord diameter in fetuses affected by Turner syndrome because lymphatic vessels are completely absent in the umbilical cord and in the placenta (4).
3. However, alterations of proteoglycan expression have been found in the skin of fetuses with Turner syndrome. It has been reported that, in fetuses with Turner syndrome, biglycan, which is encoded on chromosome X, is under-expressed and chondroitin-6-sulfate is over-expressed (5). Thus, it reasonable to assume that similar extracellular matrix modifications might also affect the Wharton’s jelly which for a large part is composed of proteoglycans.
4. Another mechanism that might explain the increased umbilical cord size is venous congestion (3). Cardiac defects and abnormalities of the great arteries are common findings in fetuses with increased nuchal translucency (6). Absent or reverse flow during atrial contraction at the level of the ductus venosus has been reported in a very high proportion of chromosomally abnormal fetuses between 11 and 14 weeks of gestation (7). As a consequence, umbilical vein congestion may cause umbilical vein dilatation, transudation of fluid into the Wharton’s jelly and enlargement of the umbilical cord size.


|
ABNORMALITIES OF CORD
MATRIX |
TRISOMY 21 |
· Alterations of the extracellular matrix are present in fetuses affected by trisomy 21, 13 and 18 (8,9) have been demonstrated in numerous studies.
· In fetuses with trisomy 21, the extracellular matrix of the nuchal skin is much richer in glucosaminoglycan (especially hyaluronan) when compared to chromosomally normal fetuses (3,5). This appears to be the consequence of a decreased degradation of hyaluronan in fetuses with trisomy 21.
TRISOMY 18 |
· In the nuchal skin of trisomy 18 fetuses, the distribution and organization of collagen types I and III is different compared to normal fetuses, resembling modification occurring with aging (10).
· In trisomy 18, most dermal fibroblasts have been found to be laminin positive and in trisomy 13 most dermal fibroblasts are collagen type IV positive (8).
· In gestational age-matched control normal fetuses, this was never found to be the case (38).
INCREASED NUCHAL TRANSLUCENCY |
An over-expression, as well as an under-expression, of different structural proteins, polysaccharides and proteoglycans of the extracellular matrix, might result in abnormal accumulation of fluid, and could explain both the increased nuchal translucency and increased umbilical cord diameter.
REFERENCES |
- Weissman A & Jakobi P. Sonographic measurements of the umbilical cord in pregnancies complicated by gestational diabetes. J Ultrasound Med 1997; 16: 691–694
- Raio L, Ghezzi F, Di Naro E et.al. Prenatal diagnosis of a ‘lean’ umbilical cord: a simple marker for fetuses at risk of being small for gestational age at birth. Ultrasound Obstet Gynecol 1999; 13: 76–80
- Von Kaisenberg CS, Nicolaides KH, Brand-Saberi B. Lymphatic vessel hypoplasia in fetuses with Turner syndrome. Hum Reprod 1999; 14: 823-6
- Benirschke K, Kaufman P. Pathology of the Human Placenta , 3rd edn. New York: Springer-Verlag, 1995: 323
- Von Kaisenberg C, Hyett J. Pathophysiology of increased nuchal translucency. In Nicolaides KH, Sebire NJ, Snijders RJM, eds. The 11-14-Week Scan . London: Parthenon Publishing, 1999: 95-114
- Pandya P. Nuchal translucency thickness. In Nicolaides KH, Sebire NJ, Snijders RJM, eds. The 11-14-Week Scan. The Diagnosis of Fetal Abnormalities . Parthenon Publishing, 1999: 14-8
- Matias A, Gomes C, Flack N, Montenegro N, Nicolaides K. Screening for chromosomal abnormalities at 11-14 weeks: the role of ductus venosus blood flow. Ultrasound Obstet Gynecol 1998; 12: 380-4
- Von Kaisenberg CS, Krenn V, Ludwig M, Nicolaides KH, Brand-Saberi B. Morphological classification of nuchal skin in human fetuses with trisomy 21, 18 and 13 at 12-18 weeks and in a trisomy 16 mouse. Anat Embryol (Berl) 1998; 197: 105-124
- Von Kaisenberg CS, Brand-Saberi B, Christ B, Vallian S, Farzaneh F, Nicolaides KH. Collagen type VI gene expression in the skin of trisomy 21 fetuses. Obstet Gynecol 1998; 91: 319-323
- Brandt-Saberi B, Epperlein HH, Romanos GE, Christ B. Distribution of extracellular matrix components in nuchal skin from fetuses carrying trisomy 18 and trisomy 21. Cell Tvolume Res 1994; 277: 465-475