|
FETAL ANEMIA |
The
most common causes of fetal anemia include:
- Maternal
red-cell alloimmunization (maternal Rh alloimmunization occurs
when a pregnant woman develops an immunological response to a paternally
derived red blood cell antigen (D) foreign to the mother and inherited by
the fetus. The antibodies may cross the placenta, bind to antigens present
on the fetal erythrocytes, and cause hemolysis. Hemolysis of the erythrocytes causes anemia in the
fetus, and if severe, may result in edema, hydrops
fetalis, and fetal death. Hemolytic disease of
the fetus/neonate can also be caused by other antigens of the Rh blood group system and by the so-called
 irregular
antigens
irregular
antigens of the non-rhesus blood group system) (1).
of the non-rhesus blood group system) (1). - Parvovirus
B19 infection.
- Feto-fetal
hemorrhage from recipient to donor occurs in 10% of cases of TTTS.
- Kell-induced
anemia.
- Anemia
in non-immune Hydrops.
PATHOPHYSIOLOGY |
It is believed that the blood velocity is increased in any
vessel of a severely anemic fetus (2).
An anemic fetus will have a raised PSV due to increased blood flow to the brain through increased cardiac output and decreased blood viscosity. It has been shown that when the fetal anemia is corrected by blood transfusion the MCA-PSV normalizes.
ULTRASOUND ASSESSMENT |
|
MCA-PV |
Doppler assessment of the MCA-PSV has been exhaustively studied in the non-invasive diagnosis of fetal anemia. |
Abnormal values greater than 1.5 MoM |
|
Liver length
(3) |
Liver length was measured in a sagittal plane on the right side of the fetus from the dome of the diaphragm to the tip of the right lobe. Blood flow velocities are more likely to be related to the degree of anemia than liver size. |
Values greater than
the 95th percentile |
|
Spleen perimeter
(4) |
The fetal spleen was visualized in a cross-section of the fetal abdomen. The perimeter was estimated by adding the longitudinal and transverse diameters and multiplying this by 1.57. Blood flow velocities are more likely to be related to the degree of anemia than spleen size. |
Values greater than
the 95th percentile |
|
IHUV maximum velocity
(5-7) |
The maximum velocity in the IHUV was measured in a cross-section of the fetal abdomen. The sample volume was placed at approximately one third of the distance between the abdominal wall and the portal vein, with the gate adjusted to the diameter of the vessel. The angle of insonation was kept under 30°, with onscreen angle correction. A steady flow velocity pattern of 5 s was obtained before freezing the image. The maximum velocity was measured by placing a caliper with the horizontal lines on the edge of the Doppler signal. |
Values greater than
the 95th percentile |
|
Tricuspid regurgitation |
Tricuspid regurgitation precedes the development of ascites and hydrops. |
Although tricuspid
regurgitation can be found in normal and non-anemic fetuses, it is always
abnormal when there is holosystolic regurgitation. |
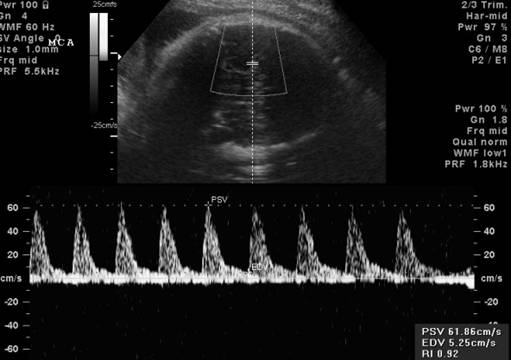
MIDDLE CEREBRAL ARTERY PEAK SYSTOLIC VELOCITY (MCA – PSV) |
In 1995, Mari et al (8) reported that MCA peak systolic velocity measurements could accurately predict fetal anemia in a series of 16 pregnancies complicated by maternal red blood cell alloimmunization.
Since then, several prospective studies have confirmed these findings (6,7,9).
Recent studies confirm earlier reports (4,6) suggesting that fetal blood flow velocity studies are superior tests to liver and spleen measurements in the prediction of fetal anemia in red blood cell alloimmunization.
Measurement of the peak systolic velocity in the middle cerebral artery (MCA-PSV) has emerged as one method of non-invasive identification of fetal anemia (10).
Sensitivity
Various studies have reported the success of Doppler scanning in fetal anemia and sensitivity has been reported as ranging from 73-100% with specificity from 71-80% (3,4,10,11).
Technique
Results of a recent study (12). indicate that any segment of the MCA, with the exception of the area close to its division into terminal branches, can be sampled with good results (the distal area of the MCA does not have good reproducibility is due to a technical factor: any minimal movement of the fetal head can displace the sample volume in one of the terminal branches). There are usually two or three terminal branches but in my experience there can be as many as five.
The MCA-PSV should be sampled at its proximal point, soon after its origin from the internal carotid artery, avoiding the need for angle correction, because measurement at this point is associated with the lowest intra- and interobserver variabilities (12).
a) at the level of the sphenoid bones;
b) color Doppler identifies the circle of Willis;
c) the image of the circle of Willis is enlarged;
d) the color box is placed around the MCA;
e) the MCA is zoomed;
f) the sample volume should be placed at the center of the vessel ;
g) the MCA flow velocity waveforms are displayed and the highest point of the waveform (PSV) is measured.
h) the waveforms should be all similar.
i) the above sequence is repeated at least three times in each fetus (12).
Variants
When the MCA is sampled, it is important to be aware and recognize the possible variants of this vessel:
· double MCA),
· the waveforms of its collaterals (lenticulostriates arteries).
|
Fetal middle cerebral artery peak systolic velocity
(MCA-PSV). Median and 1.5 multiples of the median (MoM)
values during pregnancy |
||
|
|
MCA-PSV (cm/s) |
|
|
GA (weeks) |
Median |
1.5 MoM |
|
14 |
19.3 |
28.9 |
|
15 |
20.2 |
30.3 |
|
16 |
21.1 |
31.7 |
|
17 |
22.1 |
33.2 |
|
18 |
23.2 |
34.8 |
|
19 |
24.3 |
36.5 |
|
20 |
25.5 |
38.2 |
|
21 |
26.7 |
40.0 |
|
22 |
27.9 |
41.9 |
|
23 |
29.3 |
43.9 |
|
24 |
30.7 |
46.0 |
|
25 |
32.1 |
48.2 |
|
26 |
33.6 |
50.4 |
|
27 |
35.2 |
52.8 |
|
28 |
36.9 |
55.4 |
|
29 |
38.7 |
58.0 |
|
30 |
40.5 |
60.7 |
|
31 |
42.4 |
63.6 |
|
32 |
44.4 |
66.6 |
|
33 |
46.5 |
69.8 |
|
34 |
48.7 |
73.1 |
|
35 |
51.1 |
76.6 |
|
36 |
53.5 |
80.2 |
|
37 |
56.0 |
84.0 |
|
38 |
58.7 |
88.0 |
|
39 |
61.5 |
92.2 |
|
40 |
64.4 |
96.6 |
|
G Mari et al. |
||
|
|
||
MCA-PSV can be used to diagnose fetal anemia due numerous causes.
Delle Chiaie et al.(13) and Cosmi et al. (14) reported that this parameter is useful in cases of fetal anemia secondary to parvovirus infection.
Senat et al(15) reported that MCA-PSV diagnoses anemia secondary to twin-twin transfusion syndrome (TTTS), and others have reported that MCA-PSV diagnoses anemia secondary to fetomaternal hemorrhage(16,17), and fetal hydrops (17,18).
VALUES
|
The MCA-PSV does not diagnose all cases of fetal anemia because, because in mildly anemic cases, the velocity does not necessarily change. The correlation between hemoglobin and MCA-PSV becomes more accurate as the severity of anemia increases (19).
When the anemia becomes very severe (hemoglobin levels of 1-3 g/dL), the velocity does not increase further.
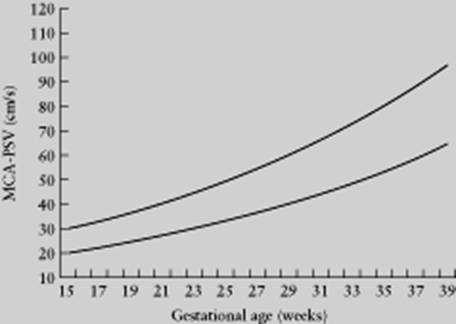
MCA peak velocities were
expressed as multiples of the median (MoM) using
previously established reference ranges, and defined as abnormal if they were
greater than 1.5 MoM (20).
If the value is below 1.5 multiples of the median (MoM). Reassess weekly.
If the value is above 1.5 MoM, assess the trend of the MCA-PSV.
Severe fetal anemia has been defined as a hemoglobin concentration of 5 SD or more below the mean for gestational age, using the reference range of Nicolaides et al (22).
In cases with parvovirus infection:
- perform an ultrasound every week for 10 weeks following the exposure.
- look for signs of anemia and evaluate the MCA-PSV.
- if the value of the velocity becomes higher than 1.5 MoM, repeat the ultrasound examination twice a week, and look for tricuspid regurgitation and ascites.
- some workers do not intervene in cases of parvovirus infection based solely on the MCA-PSV because the fetus would not necessarily become hydropic, and the anemia might resolve spontaneously without intervention.
REFERENCES
|
- G. Mari. Middle cerebral artery peak systolic velocity for the diagnosis of fetal anemia: the untold story. Ultrasound Obstet Gynecol 2005;25:323-330.
- van Dogen H, Klumper FJCM, Vandenbussche
FPHA et.al. Non invasive tests to predict fetal
anemia in Kell alloimmunized
pregnancies. Ultrasound Obstet Gynecol 2005;25:341-345.
- Roberts
AB, Mitchell JM,
- Oepkes D, Meerman RH, Vandenbussche FP, Van Kamp IL, Kok FG, Kanhai HH. Ultrasonographic fetal spleen measurements in red blood cell alloimmunized pregnancies. Am J Obstet Gynecol 1993; 169: 121-128.
- D, Brand R, Vandenbussche FP, Meerman RH, Kanhai HH. The use of ultrasonography and Doppler in the prediction of fetal haemolytic anaemia: a multivariate analysis. Br J Obstet Gynaecol 1994; 100: 680-684.
- Dukler D, Oepkes D, Seaward G, Windrim R, Ryan G. Noninvasive tests to predict fetal anemia: A study comparing Doppler and ultrasound parameters. Am J Obstet Gynecol 2003; 188: 1310-1314.
- Mari G, Deter RL, Carpenter RL, Rahman F, Zimmerman R, Moise KJ. Non-invasive diagnosis by Doppler ultrasonography of fetal anemia due to maternal red-cell alloimmunization. N Engl J Med 2000; 342: 9-14.
- Mari G, Andrignolo A, Abuhamad AZ, Pirhonen J, Jones DC, Ludomirsky A, Copel JA. Diagnosis of fetal anemia with Doppler ultrasound in the pregnancy complicated by maternal blood group immunization. Ultrasound Obstet Gynecol 1995; 5: 400-405.
- Zimmerman R, Durig P, Carpenter RJ Jr., Mari G. Longitudinal measurement of peak systolic velocity in the fetal middle cerebral artery for monitoring pregnancies complicated by red cell alloimmunization: a prospective multicentre trial with intention-to-treat. BJOG 2002; 109: 746-752.
- BabinskyA, Lapinski RH, Berkowitz RL. Prognostic factors and management in pregnancies complicated with severe kell alloimmunization: experiences of the last 13 years. Am J Perinatol 1998; 15: 695-701.
- Leggat HM, Gibson JM, Barron SL, Reid MM. Anti-Kell in pregnancy. Br J Obstet Gynaecol 1991; 98: 162-165
- Mari G, Abuhamad A, Cosmi E, Segata M, Altaye M, Akiyama M. Middle cerebral peak systolic velocity: Technique and variability. J Ultrasound Med 2005; 24: 425-430
- Delle Chiaie L, Buck G, Grab D, Terinde R. Prediction of fetal anemia with Doppler measurement of the middle cerebral artery peak systolic velocity in pregnancies complicated by maternal blood group alloimmunization or parvovirus B19 infection. Ultrasound Obstet Gynecol 2001; 18: 232-236
- Cosmi E, Mari G, Delle CL, Detti L, Akiyama M, Murphy J, Stefos T, Ferguson JE 2nd, Hunter D, Hsu CD, Abuhamad A, Bahado-Singh R. Noninvasive diagnosis by Doppler ultrasonography of fetal anemia resulting from parvovirus infection. Am J Obstet Gynecol 2002; 187: 1290-1293
- Senat MV, Loizeau S, Couderc S, Bernard JP, Ville Y. The value of middle cerebral artery peak systolic velocity in the diagnosis of fetal anemia after intrauterine death of one monochorionic twin. Am J Obstet Gynecol 2003; 189: 1320-1324.
- Mari G, Detti L. Doppler ultrasound - Application to fetal
Medicine. In The principles of ultrasonography
in obstetrics and gynecology, Manning FA ,
Fletcher A , Romero R , Jeanty P (eds). Appleton & Lange:
- Sueters M, Arabin B, Oepkes D. Doppler sonography for predicting fetal anemia caused by massive fetomaternal hemorrhage. Ultrasound Obstet Gynecol 2003; 22: 186-189.
- Cosmi E, Dessole S, Uras L, Capobianco G, D'Antona D, Andrisani A, Litta P, Ambrosini G. Middle cerebral artery peak systolic and ductus venosus velocity waveforms in the hydropic fetus. J Ultrasound Med 2005; 24: 209-213
- Mari G, Detti L, Oz U, Zimmerman R, Duerig P, Stefos T. Accurate prediction of fetal hemoglobin by Doppler ultrasonography. Obstet Gynecol 2002; 99: 589-593.
- Vyas S, Nicolaides KH, Campbell S. Doppler examination of the middle cerebral artery in anemic fetuses. Am J Obstet Gynecol 1990; 162: 1066-1068.
- Mari G, Rahman F, Oloffson P, Oczan T, Copel JA. Increase of fetal hematocrit decreases the middle cerebral artery peak systolic velocity in pregnancies complicated by rhesus alloimmunization. J Matern Fetal Med 1997; 6: 206-208
- Nicolaides KH, Bilardo CM, Campbell S. Prediction of fetal anemia by measurement of the mean blood velocity in the fetal aorta. Am J Obstet Gynecol 1990; 162: 209-212.