|
ABNORMAL WAVEFORMS IN
THE DUCTUS VENOSUS IUGR AND CHANGES IN
THE DUCTUS VENOSUS AGENESIS OF THE
DUCTUS VENOSUS |
The human fetal ductus venosus (DV) plays a major role in
the regulation of the circulation of oxygenated blood from the placenta. In
normal circumstances 20-30% of the well-oxygenated blood from the placenta gets
shunted through the DV to the left side of the heart (1). The other 70-80%
flows through the liver, mainly into the right heart and via the ductus arteriosus and the descending aorta back to the placenta.
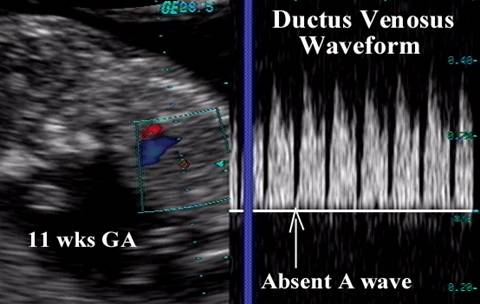
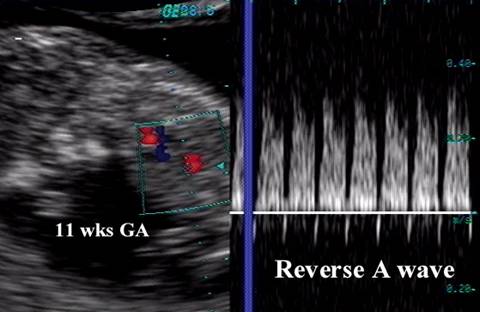
First Trimester
|
|
|
|
Absent A wave
|
|
|
Reversed A wave
|
Third Trimester
|
|
|
|
Decreased A wave
|
|
|
Reversed A wave
|

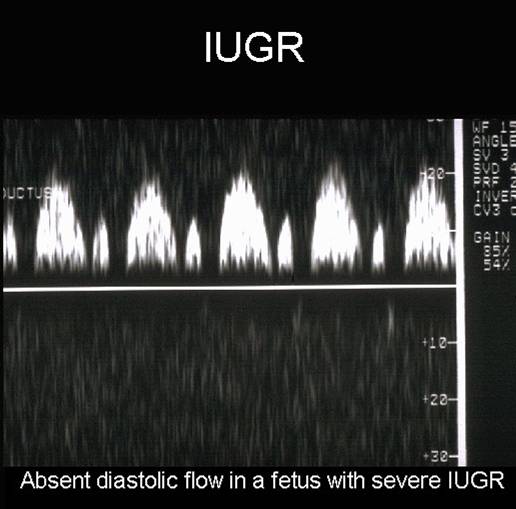
INTRAUTERINE GROWTH RESTRICTION (IUGR) |
In fetal compromise up to 70% of the umbilical venous blood gets shunted through the DV to maintain a high oxygen supply to essential organs such as the brain, heart and adrenal glands, and liver perfusion is reduced to 30% as shown in studies in animals and in the human fetus (1,11). This diversion of oxygenated blood and reduced flow to less important organs like muscles, bowel and kidney, enables the fetus to survive for a considerable period of time, especially if the fetus is under 30 completed weeks of gestation. If the oxygen supply to the myocardium reaches its limit, the myocardium stiffens and the central venous pressure increases. This can be reflected in the blood velocity pattern in the inferior vena cava, hepatic veins, and the DV. So far there have been only few publications that focus on specific changes in the venous velocimetry prior to fetal demise (8).
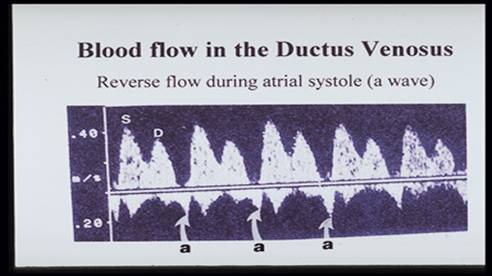
The ductus venosus
and hepatic vein (HV) velocity waveforms are analyzed for peak systolic velocity
(S), peak velocity during early diastole (D) and the maximum velocity
corresponding to atrial contraction in late diastole
(A) and also, as a new parameter, the peak end-systolic velocity (ES), to
determine the intra-atrial pressure at the end of systole.
S![]() A/S-
and S
A/S-
and S![]() ES/S-ratios
were calculated, also the percentage reversal of flow in the right HV (17).
ES/S-ratios
were calculated, also the percentage reversal of flow in the right HV (17).
|
|
|
|
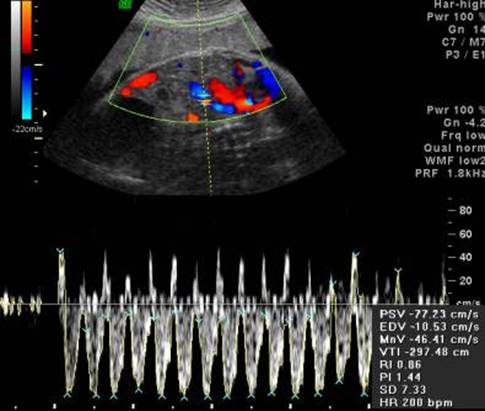
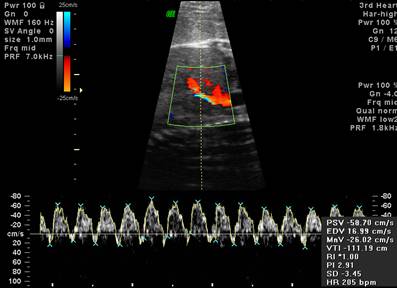
- Reverse flow in the ductus venosus is an ominous sign.
|
Reverse flow in ductus at 31 weeks – severe IUGR |
|
|
|
|
|
|
Video clip of the
Ductus Venousus - reverse A wave
|
|
|
|
|
|

- In one series (1), five fetuses with reverse flow velocity waveforms in the ductus venosus died in utero. In 18 other fetuses with abnormal umbilical and MCA waveforms (ratio >1), but without reversal of flow in the ductus venosus, no deaths occurred.
- The A wave is usually positive, however prior to 15 weeks of gestation a negative component may be recorded in normal fetuses (1).
- The highest velocities recorded in the ductus venosus are seen in diseases affecting the liver parenchyma (mitochondrial diseases, viral infetion, leukemoid infiltration and augmented erythropoietic activity). Hyperkinetic circulation (e.g. anemia) has also been associated with increased velocities in the ductus venosus (13).
- A study by Hofstaetter and coworkers (18) suggests that blood velocity waveform in the HV was an earlier predictor of intrauterine death than that of the DV. This might be due to the fact that the HV is nearer the heart and blood flow from the right liver lobe flows mainly to the right side of the heart, while that from the DV mainly to the left ventricle via the foramen ovale. The fetal left ventricle, in these pregnancies, usually has to work against a lower afterload than the right ventricle, due to brain sparing in chronic hypoxia. The difference in afterload might cause some differences in timing of signs of imminent heart failure in the two vessels. As flow from the right HV mainly enters the right ventricle, a compromised fetal state may therefore be expressed better in the HV than in the DV. Nevertheless the DV is often easier to locate because of its brightness on color Doppler and therefore it will continue to be used in clinical practice
AGENESIS OF THE DUCTUS VENOSUS |
- Rare phenomenon but has been described antenatally (2).
- The resultant return of the umbilical blood flow is via numerous vicarious pathways that bypass the liver:
- Suprahepatic connection to the IVC.
- Infrahepatic connection to the IVC.
- Rarely directly to the right atrium.
- Iliac connection.
- Cutaneous anastomosis (results in the formation of a caput medusa).
- Associated anomalies are not infrequent; fetal aneuploidy (3), focal liver necrosis and calcification (4), diaphragmatic hernia (5), hydrops and cardiovascular anomalies (6,7) have been reported.
- Absence of the ductus venosus may be compatible with normal fetal development without significant disturbance of fetal circulation and oxygenation (3).
- A recent report in monochorionic twins resulted in severe hemodynamic consequences that contributed to volume overload in one twin producing a clinical picture that mimicked the twin-twin transfusion syndrome.
- There are numerous reports of fetal demise associated with agenesis of the ductus combined with fetal hydrops, asphyxia, vascular and cardiac anomalies. This suggests that normal development depends on the presence of the duct (14-16), although some workers argue that these fetuses are examined because they are sick or died.
|
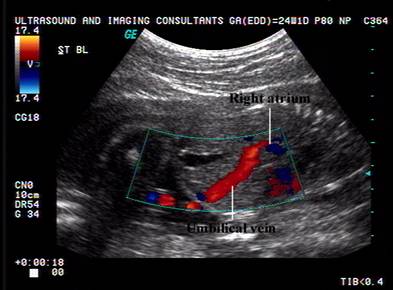
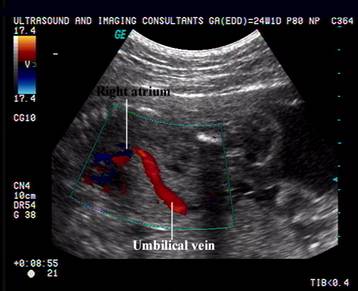
Absent Ductus Venosus. Aberrant insertion of umbilical
vein into right atrium of the heart. This was the pump twin of an acardiac twin pregnancy. |
|
|
|
|
|
|
|


TWIN-TWIN TRANSFUSION |
- Mean velocity decreased with significant increase in PI in recipients (8). Donors and recipients exhibit reversal of end diastolic velocity in the umbilical artery with abnormal ductus venosus flow velocity indices (9).
CONGENITAL HEART DISEASE |
- Ductus venosus index is not affected in pathology involving the left atrium and ventricle (hypoplastic left heart syndrome) (10).
- Abnormal hemodynamics have been demonstrated in right ventricular pathology (11).
REFERENCES |
- Kiserud T. Hemodynamics of the ductus venosus. Eur J Obstet Gynecol Reprod Biol 1999;84:139-147.
- Shih JC, Shyu MK, Hsieh MH et.al. Agenesis of the ductus venosus in a case of monochorionic twins which mimics twin-twin transfusion syndrome. Prenat Diagn 1996;16:243-246.
- Gembruch U, Baschat AA, Caliebe A, Gortner L. Prenatal diagnosis of ductus venosus agenesis: a report of two cases and review of the literature. Ultrasound Obstet Gynecol 1998;11:185-189.
- Cohen SB, Lipitz S, Mashiach S et.al. In utero ultrasonograhic diagnosis of an aberrant umbilical vein associated with fetal hepatic hyperechogenicity. Prenat Diagn 1997;17(10):978-982.
- Strouse PJ, Di Pietro MA, Barr M Jr. Pitfall: anomalous umbilical vein and absent ductus venosus in association with right congenital diaphragmatic hernia. Pediatr Radiol 1997;27(8):651-653.
- Siven M, Ley D, Hagerstrand I, Svenningsen N. Agenesis of the ductus venosus and its correlation to hydrops fetalis and the fetal hepatic circulation: case report and review of the literature. Pediatr Pathol Lab Med 1995;15(1):39-50.
- Jorgensen C, Andolf E. Four cases of absent ductus venosus: three in combination with sever hydrops. Fetal Diagn Ther 1994;9(6):395-397.
- Hecher K, Ville Y, Snijders R et.al. Doppler studies of the fetal circulation in twin-twin transfusion syndrome. Ultrasound Obstet Gynecol 1995;5:318-324.
- Rizzo G, Capponi A, Arduini D et.al. Ductus venosus velocity waveforms in appropriate and small for gestational age fetuses. Early Hum Dev 1994;39:15-26.
- DeVore GR, Horenstein J. Ductus venosus index: A method for evaluating right ventricular preload in the second trimester fetus. Obstet Gynecol 1993;3:338-342.
- Kiesreud T, Eik-Nes SH, Hellevik LR et.al. Ductus venosus blood velocity changes in fetal cardiac diseases. J Mat Fetal Invest 1993;3:15-20.
- Goncalves LF, Romero R, Silva M et.al. Reverse flow in the ductus venosus: An ominous sign. Am J Obstet Gynecol 1995;172(1):266.
- Kiserud T. The ductus venosus. Semin Perinatol 2001;25(1):11-20.
- Jorgensen G, Andolf E. Four cases of absent ductus venosus: three in combination with severe hydrops fetalis. Fetal Ther 1994;395-397.
- Siven M, Ley D, Hagenstrand I et.al. Agenesis of the ductus venosus and its correlation to hydrops fetalis and fetal hepatic circulation. Pediatr Pathol Lab Med 1995;39-50.
- Gembruch U, Baschat AA, Gortier L. Prenatal diagnosis of ductus venosus agenesis: a report of two cases and review of the literature. Ultrasound Obstet Gynecol 1998;11:185-189.
- Reed KL, Appleton CP, Anderson CF et.al. Doppler studies of the vena cava flows in human fetuses. Circulation 1990;81:498-505.
- Hofstaetter C, Gudmundsson S, Hansmann. Venous doppler velocimetry in the surveillance of severly compromised fetuses. Ultrasound Obstet Gynecol 2002;20:233-239.