|
ABNORMAL WAVEFORMS IN
THE UMBILICAL ARTERY (1-18) |
The resistance in the umbilical
artery is defined semiquantitatively in blood flow classes according to
reference 18.
BFC 0: normal umbilical
artery blood velocity;
BFC I: increased PI, but still
forward flow in diastole;
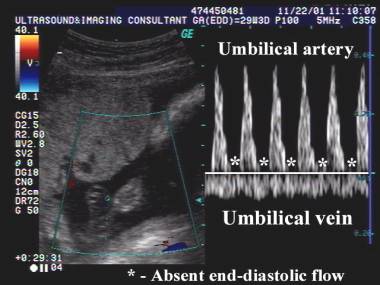
BFC II: absent flow in
end-diastole;
BFC III: absent flow
throughout diastole or reversal of flow.
The
use of the modality of umbilical artery doppler is based on the premise that
placental insufficiency results in adverse outcome such as fetal growth
restriction, fetal asphyxia or perinatal mortality, and that this abnormality
can be defined using doppler sonography (1-12). Several authors have suggested
that the severity of fetal compromise can be predicted by the extent of the
abnormalities on the doppler studies (6). Marsal and associates (7) have
demonstrated an association between abnormal fetal blood flow and long-term
neurodevelopmental impairment. Valcamonico and co-workers (8) have demonstrated
that growth restricted infants who experienced absent or reversed end-diastolic
flow in the umbilical artery waveform, suffer a higher incidence of long-term
permanent neurological damage relative to pregnancies in which some
end-diastolic flow was documented.
·
Doppler use is associated with a reduction in the incidence of
intrauterine death in normally formed fetuses:
o
Giles and Bisits (1993) (9) evaluated umbilical
artery velocimetry in the management of high-risk pregnancies. Meta-analysis of
6 published pier-reviewed and randomized controlled trials; 2102 patients in
doppler group and 2133 patients in control (non-doppler) group. Results showed
that there was a reduction in intrauterine death in normally formed fetuses,
with a relative risk of 0.54 and a confidence interval of 0.32-0.89, without a
concomitant increase in inappropriate obstetric intervention.
o
Alfirevic and Neilson (1995) (10) reached the same conclusions.
·
The use of umbilical artery doppler in high-risk pregnancies appears to
result in a reduction in antenatal admissions, inductions of labor, cesarean
sections for fetal distress, and perinatal mortality (10).
o
A meta-analysis of 8 published and peer-reviewed
randomized trials of 6838 patients revealed that umbilical artery doppler
studies significantly decreased perinatal mortality with an odds ratio of 0.66
and a CI of 0.46-0.94. The authors concluded that there was sufficient data to
indicate that the use of doppler velocimetry in high-risk pregnancies reduced
perinatal morbidity and that no further studies were necessary to substantiate
this recommendation (11).
o
Neilson and Alfirevic (12) reviewed 11 randomized
controlled trials in 7000 high-risk pregnancies (randomized to doppler versus non-doppler). Doppler
ultrasound (especially in pregnancies complicated by hypertension of presumed
fetal growth reduction) was associated with a trend towards a reduction in
perinatal deaths (odds ratio 0.71, 95% CI = 0.50-1.01). The use of doppler was
also associated with fewer inductions of labor (odds ratio 0.83, 95% CI = 0.43-0.72),
without reports of adverse perinatal effects. No differences were found in the
rates of intrapartum fetal distress or cesarean delivery. They concluded that
the use of doppler studies is likely to reduce perinatal death rates.
- IUGR.
- The growth-restricted fetus is at risk for adverse perinatal outcome.
- In cases of placental insufficiency, a higher placental vascular resistance results in a decreased diastolic component of the umbilical artery waveform (1,2). Placental pathology includes vascular sclerosis and obliteration of tertiary stem villi, villous stromal hemorrhage, hemorrhagic endovasculitis, and abnormally thin-walled fetal stem vessels (5).
- PI, RI and S/D ratio all increase.
- Diastolic velocities decrease, become absent, and is later reversed. If placental insufficiency is mild and does not progress, a decreased diastolic velocity remains constant and never becomes absent or reversed.
|
|
Video clip of Absent end-diastolic
flow Video clip of absent
end-distolic flow
|
|
|
|
|
|

- Serial measurements offer more information than a single study as ratios may normalize with treatment or advancing gestation (3).
- Non-randomized studies.
- Randomized studies.
- Small-for-gestational-age
(SGA) fetus.
- The most common definition for growth restriction is weight less than the 10th percentile for gestational age. However not all infants whose birth weight is below the 10th percentile have been exposed to some pathological process that leads to growth restriction. Most small babies are constitutionally small and healthy. Differentiating a symmetrical growth restricted baby from a health SGA baby is still a challenge in obstetrics.
- Sonographic biometry is more sensitive than umbilical artery waveforms and ratios in identifying SGA fetuses (4).
- Doppler identifies the SGA at risk for poor perinatal outcome rather than the constitutionally small but otherwise normal fetus.
- Baschat and Weiner (13) evaluated 308 fetuses with ultrasonographic weight estimate less than the 10th percentile or an abdominal circumference less than the 2.5th percentile for gestational age with doppler of the umbilical artery. 138 fetuses had elevated S/D ratios (>90th percentile for gestational age) and found that abnormal doppler studies were associated with lower arterial and venous pH values, an increased likelihood of intrapartum fetal distress, more admissions to neonatal ICU and a higher incidence of respiratory distress syndrome. No fetus with normal doppler flow measurements was delivered with a metabolic academia associated with chronic hypoxemia. The authors suggest that antenatal surveillance is unnecessary in fetuses with suspected growth restriction if the umbilical artery doppler studies are normal. Other groups of workers have concluded that small fetuses with normal umbilical artery doppler studies are more likely to be constitutionally small and healthy rather than growth restricted and sick (14, 15).
- Low-risk pregnancies.
- Goffinet et.al. (16) published a meta-analysis of the use of umbilical artery doppler velocimetry in low-risk, unselected pregnancies. 11,375 pregnancies participated in 4 randomized controlled trials. Systematic use of umbilical artery doppler had no statistically detectable effect on perinatal deaths in unselected populations (odds ratio 1.28; 95% CI 0.61-2.67), low risk populations (odds ratio 0.51; 95% CI 0.20-1.29), or overall for the 4 trials (odds ratio 0.90, 95% CI = 0.50-1.60), nor was there any significant effect on stillbirths (global odds ratio 0.94; 95% CI 0.42-1.98). They conclude that umbilical artery doppler studies in low risk patients is unlikely to be beneficial.
- Bricker and Nelson (17) reviewed 5 trials to masses the effects on the practice of obstetrics and pregnancy outcome of routine doppler ultrasound use in unselected and low-risk pregnancies (14,388 women). The authors reported in the Cochrane Library that based on existing evidence, routine doppler ultrasound in low-risk or unselected populations does not confer benefit on mother or newborn.
- Lupus Anticoagulant..
REFERENCES |
- Trudinger BJ, Stevens D, Connelly A et.al. Umbilical artery flow velocity waveforms and placental resistance: The effects of embolization of the umbilical circulation. Am J Obstet Gynecol 1987;157:1443-1449.
- Devoe LD, Gardner P, Dear C et.al. The significance of increasing umbilical artery systolic-diastolic ratios in third trimester pregnancy. Obstet Gynecol 1992;80:684-687.
- Trudinger BJ, Cook CM, Giles WB. Fetal umbilical artery velocity waveforms and subsequent neonatal outcome. Br J Obstet Gynaecol 1991;98:378-384.
- Chambers SE, Hoskins PR, Haddad NG et.al. A comparison of fetal abdominal circumference measurements and Doppler ultrasound in the prediction of Small for gestational age babies and fetal compromise. Br J Obstet Gynaecol 1989;96:803-808.
- Salafia CM, Pezzullo LC, Minior VK et.al. Placental pathology of absent and reversed end-diastolic flow in growth-restricted fetuses. Obstet Gynecol 1997;90:830-836.
- Divon MY. Umbilical artery doppler velocimetry: clinical utility in high-risk pregnancies. Am J Obstet Gynecol 1996;174:10-14.
- Marsal K, Gudmundsson S,
Stale H. Doppler velocimetry in monitoring fetal health during late
pregnancy. In: Kurjak A, Chervenak F (eds): The fetus as a patient.
- Valcamonico A, Danti L, Frusca T et.al. Absent end-diastolic velocity in the umbilical artery: Risk of neonatal morbidity and brain damage. Am J Obstet Gynecol 1994;170:796-801.
- Giles WB, Bisits A. Clinical use of doppler in pregnancy: information from six randomized trials. Fetal Diagn Ther 1993;8:247-255.
- Alfirevic A, Nielson JP. Doppler ultrasonography in high-risk pregnancies: Systemic review with meta-analysis. Am J Obstet Gynecol 1995;172:1379-1387.
- Divon MY. Randomized controlled trials of umbilical artery doppler velocimetry: How many are too many? (editorial). Ultrasound Obstet Gynecol 1995;6:377-379.
- Nelson JP, Alfirevic Z.
Doppler ultrasound for fetal assessment in high-risk pregnancies (Cochrane
review), in The Cochrane Library, Issue 4, 2000.
- Baschat AA, Weiner CP. Umbilical artery doppler screening for detection of the small fetus in need of antepartum surveillance. Am J Obstet Gynecol 2000;182:154-158.
- Burke G, Stuart B, Crowly P et.al. Is intrauterine growth retardation with normal umbilical artery blood flow a benign condition? BMJ 1990;300:1044-1045.
- Pattinson RC, Norman K, Odendaal HJ. The role of doppler velocimetry in the management of high risk pregnancies. Br J Obstet Gynaecol 1994;101:114-120.
- Goffinet F, Paris-Llado J, Nisand I et.al. Umbilical artery doppler velocimetry in unselected and low-risk pregnancies: A review of randomized controlled trials. Br J Obstet Gynaecol 1997;104:425-430.
- Bricker L, Neilson JP.
Routine doppler ultrasound in pregnancy (Cochrane review), in The Cochrane
library, Issue 3, 2000.
- Laurin J, Lingman G, Marsal K et.al. Fetal blood flow in pregnancy complicated by intrauterine growth retardation. Obstet Gynecol 1987;69:895-902.