|
PERIGESTATIONAL
HEMORRHAGE (PGH) |
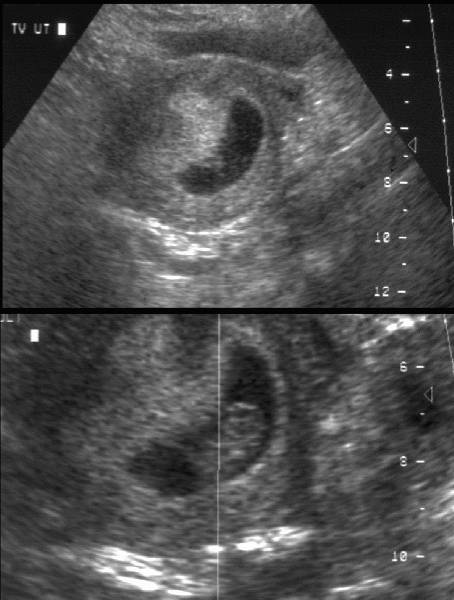
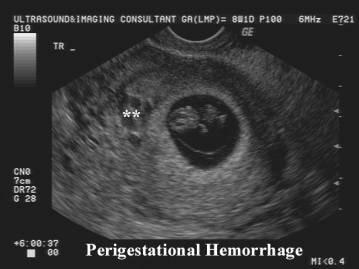
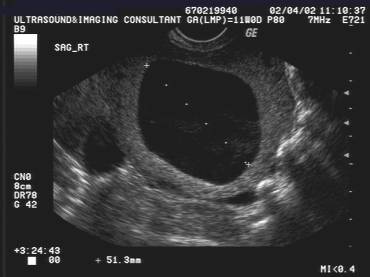
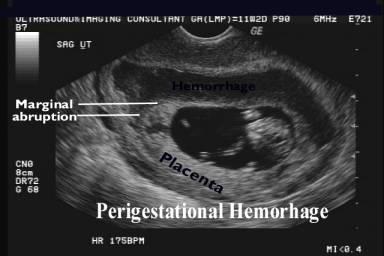
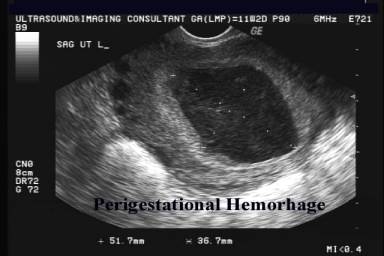
PGH are crescent-shaped, echo-free areas between the chorionic membrane and the myometrium (1).
- Most common source of vaginal bleeding during pregnancy.
- Up to 20% of women with threatened abortion.
- Originates from the chorion frondosum (bleeding typically occurs between the decidua basalis and chorion frondosum or chorionic leave).
- May present with:
- External bleeding + no significant intrauterine hematoma.
- Formation of a retroplacental or marginal hematoma +/- external bleeding.
- Formation of a submembranous hematoma away from the site of the developing placenta.
- Overall, the presence of an
IUH has been associated with a 4-33% rate of miscarriage depending on the
gestational age at which the complication was described (2).
- Vaginal bleeding in very
early pregnancy (i.e. before 6 weeks' gestation) does not seem to be
associated with any immediate or long-term consequences (3).
- Threatened miscarriage
symptoms at 7-12 weeks, even in the presence of detectable fetal cardiac
activity, is not only associated with:
- a 5-10% miscarriage rate
before 14 weeks of gestation
- adverse
pregnancy outcome at later gestations (4-7); (bleeding in the second half
of the first trimester are at higher risk of PPROM and preterm labor).
- These risks are
independent of the presence or absence of an IUH on the initial
ultrasound examination and would suggest that threatened miscarriage in
the first trimester is a risk factor for adverse pregnancy outcome
regardless of the ultrasound findings.
ULTRASOUND |
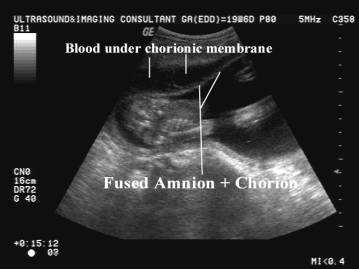
- Separation of the chorioamniotic membrane from the uterine wall by a fluid collection. Visualization of the usually inapparent chorioamniotic membrane as a fine linear echo in the gestational sac becomes evident.
|
|

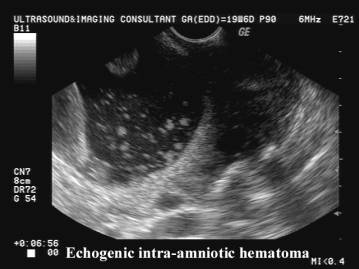
- Acute hemorrhage is usually echogenic.
|
|
- Hemorrhage becomes hypoechoic with subsequent liquefaction of the clot.
|
|
|
|
|
|


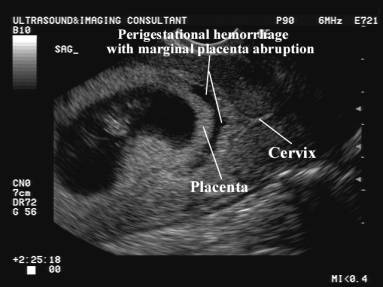
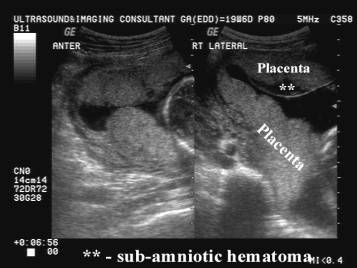
- Area of hemorrhage usually extends under the margin of the placenta.
|
|

- Area of hemorrhage is never found over the fetal surface of the placenta (unlike chorio-amniotic separation).
|
|
|
|
|
|
|
|




- Active hemorrhage may be sonographically demonstrated on color and power doppler.
|
|
|

- Hemorrhage may break through the membranes and extend into the amniotic cavity – intra-amniotic hemorrhage.
|
|
|
|
|
|

|
|
Video image of Perigestational Hemorrhage Video image of Perigestational Hemorrhage – active bleeding
|
|
|
|
|
|

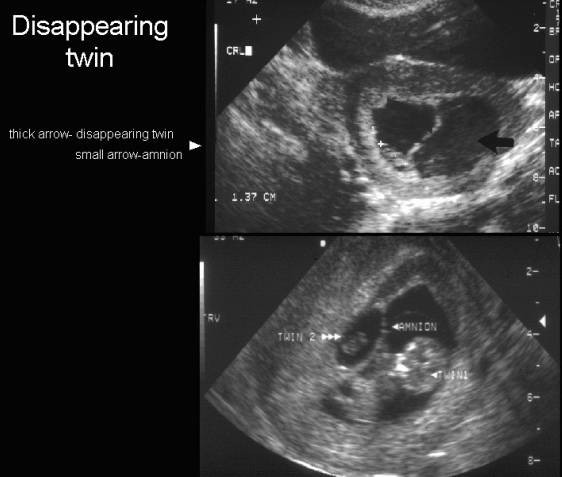
DIFFERENTIAL DIAGNOSIS |
- Disappearing twin.
|
|
|
|
|
|

OUTCOME OF PREGNANCY IS DEPENDENT ON: |
- Size of hemorrhage (small ones usually resolve without sequelae).
- volume = length(cm) X width(cm) X height(cm) X 0.5
- volume = < 1/4 of gestational sac or < 60ml the pregnancy is likely to progress (1).
|
|
|
|
|
|


·
In
the past, much emphasis has been placed on the volume of an intrauterine hematoma (PGH) (8-10) or on the presence of vaginal
bleeding (9) but not on the location of the hemorrhage. It appears that if the
bleeding occurs at the level of the definitive placenta (under the cord
insertion) it may result in placental separation and subsequent abortion.
Conversely, a PGH that only detaches the membrane a distance away from the cord
insertion can probably reach a significant volume before it affects normal
pregnancy development by a direct volume pressure effect. The presence of a hematoma may also be associated with a chronic inflammatory
reaction in the decidua, resulting in persistent myometrial activity and expulsion of the pregnancy (11).
COMPLICATIONS |
- Fetal demise.
- Disseminated intravascular coagulopathy due to tissue breakdown in large, chronic retroplacental hematomas (2).
ETIOLOGY |
- Seen in asymptomatic patients.
- Patients with bleeding disorders.
- Trauma including amniocentesis.
- Patients with vasculopathies e.g. maternal hypertensive states.
REFERENCES |
- Sauerbrei
EE, Pham DH. Placental abruption and subchorionic
hemorrhage in the first half of pregnancy:
- Spirt BA, Kagan EH, Aubry RH. Clinically silent retroplacental hematoma: Sonographic and pathologic correlation. J Clin Ultrasound 1981;9:203.
- Pearlstone M, Baxi L. Subchorionic hematoma: a review. Obstet Gynecol Surv 1993; 48: 65-68.
- Harville EW, Wilcox AJ, Baird DD, Weinberg CR. Vaginal bleeding in very early pregnancy. Hum Reprod 2003; 18: 1944.
- Tongsong
T, Srisomboon J, Wanapirak
C, Sirichotiyakul S, Pongsatha
S, Porisuthikul T. Pregnancy outcome of
threatened abortion with demonstrable fetal cardiac activity: a cohort
study. J Obstet
Gynecol
- Yang J, Hartmann KE, Savitz DA, Herring AH, Dole N, Olshan AF, Thorp JM Jr. Vaginal bleeding during pregnancy and preterm birth. Am J Epidemiol 2004; 160: 118-125.
- Weiss JL, Malone FD, Vidaver J, Ball RH, Nyberg DA, Comstock CH, Hankins GD, Berkowitz RL, Gross SJ, Dugoff L, Timor-Tritsch IE, D'Alton ME; FASTER Consortium. Threatened abortion: a risk factor for poor pregnancy outcome, a population-based screening study. Am J Obstet Gynecol 2004; 190: 745-750.
- Mantoni M, Pedersen JF. Intrauterine haematoma - an ultrasonic study of threatened abortion. Br J Obstet Gynaecol 1981; 88: 47-51.
- Ball RH, Ade CM, Schoenborn JA, Crane JP. The clinical significance of ultrasonographically detected subchorionic hemorrhages. Am J Obstet Gynecol 1996; 174: 996-1002
- Abu-Yousef MM, Bleicher JJ, Williamson RA, Weiner CP. Subchorionic hemorrhage: sonographic diagnosis and clinical significance. Am J Roentgenol 1987; 149: 737.
- Salafia CM, Lopez-Zeno JA, Sherer DM, Whittington SS, Minior VK, Vintzileos AM. Histologic evidence of old intrauterine bleeding is more frequent in prematurity. Am J Obstet Gynecol 1995; 173: 1065-1070