|
TWIN-TWIN TRANSFUSION
SYNDROME (TTTS) |
Definition is not yet well defined but the most acceptable criteria is discordant amniotic fluid in the sacs of twins in the mid-trimester of pregnancy. This definition may be inaccurate unless oliguria and oligohydramnios develops in the donor and polyuria and polyhydramnios develops in the recipient twin. The twins are of the same sex however size discrepancy is frequent but not mandatory.
- Complicates 15% (4-35%) of monochorionic pregnancies (1).
- Accounts for 17% of perinatal mortality (2).
- Accounts for 12% of neonatal deaths (2).
- Accounts for 8.4% of infant deaths in twins (3-10 times higher than singletons) (2).
- Mortality is 2-3 times higher in monochorionic than in dichorionic twins (3).
- Neuro developmental abnormalities are 6-8 times more frequent in twins than in singletons. This is not entirely explained by their low birth weight and prematurity (3,4).
- Expectant management in TTS presenting prior to 28 weeks has a 80-100% perinatal mortality (1,5).
- Intrauterine demise of one twin in TTS is associated with a 3-10 times increase in neurological morbidity (6):
- Cerebral
(26% of surviving twins with a 12% mortality) (7). - Renal.
- Most workers seem to agree that the above diagnostic criteria may be present, but the diagnosis should be restricted to monochorionic twins with gross discordance of amniotic fluid volume in the second or early third trimester (8).
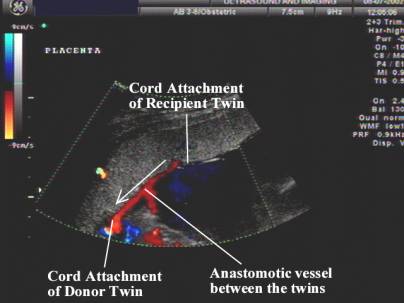
VASCULAR ANASTOMOSES IN MONOCHORIONIC TWINS |
Three types of vascular anastomoses are described:
- Artery to Artery:
- These anastomoses seem to protect against TTTS by providing a conduit for equalizing differences in mean arterial pressure in the twins. Compensatory flow occurs through these artery-artery anastomoses as a result of a hemodynamic imbalance due to the arterio-venous anastomoses.
- Recipient becomes hypertensive due to increased circulating blood volume and compensatory flow occurs in artery-artery and vein-vein anastomoses.
- Usually end-to-end anastomoses.
- Do not communicate with placental parenchyma.
- Bi-directional pulsatile spectral doppler waveforms.
- They are not strictly anastomoses as there are capillaries present, but represents a shared cotyledon with an unpaired artery from one twin, penetrating the chorionic plate next to an unpaired vein from the other twin.

- Artery to Vein:
- These are the “deep anastomoses” but are seen at fetoscopy.
- These are called the “deep anastomoses” but really means unpaired artery and vein pierce the chorionic plate in close proximity to each other and supply a cotyledon. The artery and vein are the only vessels supplying the cotyledon and course through a common foramen to each cotyledon.
- These anastomoses are thought to be responsible for TTTS.
- There is an increased risk of TTTS when there is a paucity of vascular anastomoses (artery-artery and vein to vein). A paucity of these anastomoses tend to make the arterio-venous anastomoses more unbalanced.
- May be difficult to detect antenatally.

- Vein to Vein:
- Associated with a poorer prognosis in monochorionic twins.
- Antenatal detection is very difficult.
REFERENCES |
- Pattern RM, Mack LA, Harvey D et.al. Disparity of amniotic fluid volume and fetal size: Problem of the stuck twin - US studies. Radiology 1989;172:153-157.
- Steinberg LH, Hurley VA, Desmedt E et.al. Acute polyhydramnios in twin pregnancies. Aust NZJ Obstet Gynecol 1990;30:196-200.
- Ville Y. Opinion. Monochorionic twin pregnancies: "les liaisons dangereuses". Ultrasound Obstet Gynecol 1997;10:82-85.
- Williams K, Hennessy E, Alberman E. Cerebral palsy: effects of twinning, birthweight and gestational age. Arch Dis Child 1996;75:F178-182.
- Mahony BS, Petty CN, Nyberg DA et.al. The stuck twin phenomenon: ultrasonographic findings, pregnancy outcome and management with serial amniocentesis. Am J Obstet Gynecol 1990;163:1513-1522.
- Peterson B, Nelson KB, Watson L et.al. Twins, triplets, and cerebral palsy in births in western Australia in the 1980's. Br Med J 1993;307:1239-1243.
- Okamura K, Murotsuki J, Tanigawara S et.al. Funipuncture for evaluation of hematologic and coagulation indices in the surviving twin following co-twins death. Obstet Gynecol 1994;83:975-978.
- Frisch L, Arava J, David H et,al, Severe twin-to-twin transfusion syndrome: a new sonographic feature of the placenta. Ultrasound Obstet Gynecol 1997;10:145-146.