AQUEDUCTAL STENOSIS
|
Probably develops around 15-17 postmenstrual weeks (during the period of
rapid elongation of the mesencephalon and constriction of the aqueduct). It is
the most common cause of fetal hydrocephalus (33-43%).
ETIOLOGY |
- Sporadic - external compression in the region of the third ventricle.
- Viral infection.
- Localized bleeding.
- Congenital stenosis.
- Localized defect or as a consequence of generalized disruption of brain formation.
- Inherited:
·
X-linked.
o Transmitted through female carriers to affected males. Typical history would be a mother who had brothers that have hydrocephalus.
o Caused by a mutation in the gene at Xq28 encoding for L1 (a neural cell adhesion molecule). Mutations in this gene are also responsible for other syndromes with clinical overlap that are referred to as the X-linked hydrocephalus spectrum. These syndromes include MASA (mental retardation, aphasia, shuffling gait, adducted thumbs), complicated X-linked spastic paraplegia (SP1), X-linked mental retardation-clasped thumb (MR-CT) syndrome, and some forms of X-linked agenesis of the corpus callosum.
o Dilated lateral and third ventricles (usually severe).
o Male fetus.
o Adducted thumb (44% of cases).
o Ultrasound may be normal at 18 weeks (ventriculomegaly usually evident by 16-18 weeks but may only become evident later).
o High rate of stillbirth and perinatal mortality. Survivors have significant perinatal mortality.
o Recurrence risk = 50% of males.
·
Autosomal recessive.
o Male and females affected in the same family.
ULTRASOUND |
·
Dilatation of lateral ventricles (atrium
>15mm).
·
Dilatation of third ventricle.
·
Variable dilatation of the aqueduct may be
demonstrated.
·
Normal fourth ventricle.
· Normal cerebellum and cisterna magna.
· Adducted thumb in X-linked type.
|
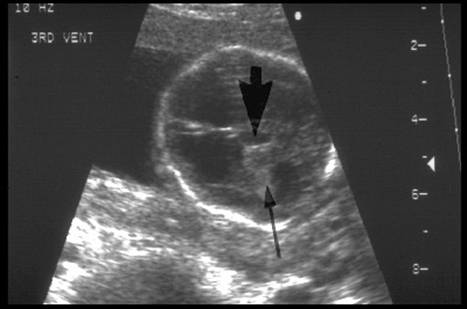
Hydrocephalus: Large 3rd
ventricle (short arrow); Dilated Lateral Ventricle |
|
|
|
|
|
Normal 4th Ventricle,
cisterna magna and cerebellum |
|
|
|
|
|
Dilated third ventricle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adducted
thumbs – X-linked |












|
|
Video clip of Aqueductal Stenosis
|
|
|
|
|
|

REFERENCES |
1. Chervenak FA, Berkowitz RL, Romero R, et.al. The diagnosis of fetal hydrocephalus. Am J Obstet Gynecol 1983;147:703-16.
2. Fransen E, Vits L, Van
3. Varadi V, Toth Z, Torok O, Papp Z. Heterogeneity and recurrence risk for congenital hydrocephalus (ventriculomegaly): a prospective study. Am J Med Genet 1998;29:305-10.
4. Kenwick S, Jouet M, Donnai D. X-linked hydrocephalus and MASA syndrome. J Med Genet 1996;33:59-65.
5. Fransen E, Vits L, Van
6. Cardoza JD, Goldstein RB, Filly RA. Exclusion of fetal ventriculomegaly with a single
measurement: the width of the lateral ventricular atrium. Radiology 1988;169:711-4.
7. Timor-Tritsch IE, Monteagudo A, Haratz-Rubinstein N,
Levine RU. Transvaginal sonographic detection of adducted thumbs,
hydrocephalus, and agenesis of the corpus callosum at 22 postmenstrual weeks:
the masa spectrum or L1 spectrum. A case report and a review of the literature.
Prenat Diagn 1996;16:543-8.
8. Jouet M, Kenwrick S.: Gene analysis of L1 neural cell adhesion molecule in prenatal diagnosis of hydrocephalus. Lancet 1995;345;161-2.