|
VEIN OF GALEN AVM |
Midline arterio-venous malformation (AVM) between choroidal and/or quadrigeminal arteries and a single median venous sac. There are multiple communications between the vein of Galen and systemic arteries (carotid and vertebrobasilar systems).
Embryological development of these non-proliferative vascular malformations are unknown. Some authors believe it results from the persistence of the prosencephalic vein of Markowski (1) and not the vein of Galen per se (2). Vascular anatomy of the aneurysm has wide variations of arteriovenous connections. It is usually supplied by choroidal branches from the posterior cerebral artery and occasionally from the transmesencephalic arteries. Venous drainage is far more complicated. Normally the vein of Galen drains into the confluence of sinuses (junction of straight, superior sagittal, and both transverse sinuses), however the straight sinus is absent or thrombosed in cases of aneurysm of the vein of Galen. The aneurysm therefore usually drains into a falcine sinus that extends directly into the superior sagittal sinus, rather than directly into the confluence (3,4).
- Diagnosis usually made in the third trimester (2/3 of cases diagnosed after 34 weeks gestation and 1/3 of cases diagnosed in second trimester)
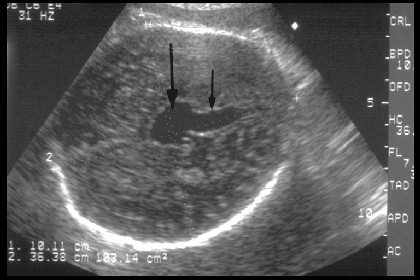
- Posterior, midline or slightly lateral anechoic structure (3).
- Supratentorial, and runs from the splenium of the corpus callosum above the cerebellum all the way to the bony cranium posteriorly.
- Posterior to the third ventricle but does not communicate with it.
- Drains into the straight sinus, which may be normal or dilated. ("Keyhole appearance") (4).
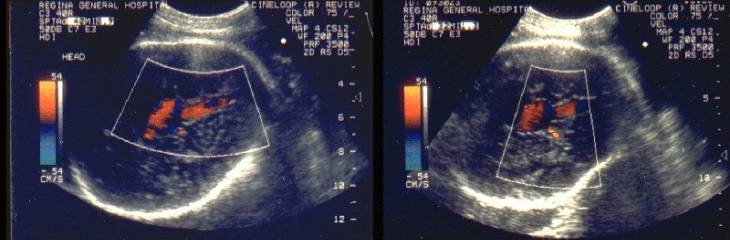
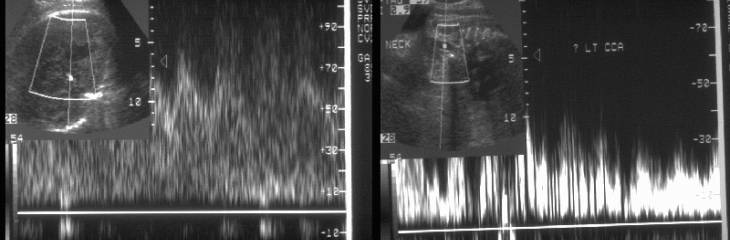
- Pulsed and color Doppler, effectively establishes the vascular nature of the lesion. Blood supply is variable; the posterior cerebral, superior cerebellar and/or anterior cerebral arteries may supply arterial blood.
- Turbulent flow is usually present within the lesion and may have arterial and/or venous flow depending on the area within the lesion that is sampled.
vessels. Visualization of blood flow including arterial feeders and venous drainage may be improved by employing color power angiography (3,7).- Associated anomalies (in 67% of fetuses)(3):
- Ventriculomegaly (?
due to mass effect and compression of the aqueduct or abnormal spinal
fluid dynamics).
Compression of the cerebral cortex by the ventriculomegaly in combination with the “steal” phenomenon may result in cerebral infarction and leukomalacia) (4) - Cardiomegaly ± ventricular wall hypertrophy (64%), ± cardiac failure.
- Neck vessels enlarged and distended (33%). This is reported as a pathognomonic sign (6).
- Vascular steal syndrome (reverse flow in the aortic arch affecting left subclavian blood flow) (8,9).
- Pulmonary
hypertension may occur due to the large systemic shunt.
Ballantyne Syndrome (10); fetal and maternal edema and placentomegaly. - Single umbilical artery; chorioangioma of the placenta and other variable anomalies have been reported.
- Other features may include, tricuspid insufficiency, polyhydramnios, pericardial or pleural effusion, edema and ascites.
|
|
Gray-scale image |
|
|
Color flow and pulsed doppler
waveforms |
||
|
|
||
|
|
||
|
|
CT scan – post-natal scan |
|
|
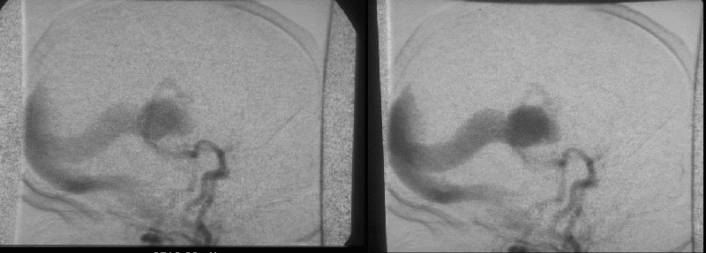
Post-natal angiogram |
||
|
|
||

|
|
Video clip of a
Vein of Galen AVM.
|
|
|
|
|
|

DIFFERENTIAL DIAGNOSIS |
These include other cystic lesions of the brain such as arachnoid cyst, porencephalic cyst as well as pineal tumor, intracerebral hematoma and choroid plexus papilloma. The classical doppler findings effectively excludes all the other possibilities.
PROGNOSIS |
- Poor when associated with hydrops or hydrocephalus (8,9).
- There are two reports of serial examinations that have shown that in later stages of pregnancy the vein of Galen aneurysm expands and cardiac decompensation develops (10,11).
- The prognosis appears to be related to the appearance of heart failure and not on the size of the lesion.
REFERENCES |
- Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: embryologic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology 1989;31:109-128.
- Evans A, Twining P. Case report: in utero diagnosis of a vein of Galen aneurysm using color flow doppler. Clin Radiol 1991;44:281-282.
- Lee T –H, Shih J –C, Peng S –F, Lee C–N, Shyu M –K, Hsieh F –J. Prenatal depiction of an aneurysm of angioarchitecture of the vein of Galen with three-dimensional color power angiography. Ultrasound Obstet Gynecol 200;15:337-340.
- Romero R, Pilu G, Jeanty P, Ghidini A, Hobbins JC. Prenatal diagnosis of Congenital Anomalies: The central nervous system. Appleton and Lange 1988, pp77-79.
- Sepulveda W, Platt CC, Fisk NM. Prenatal diagnosis of cerebral arteriovenous malformation using color Doppler ultrasound: a case report and review of the literature. Ultrasound Obstet Gynecol 1995;6:282-286.
- Strayss S, Weinraub Z, Goldberg M. Prenatal diagnosis of vein of Galen arteriovenous malformation by duplex sonography. J Perinatol Med 1991;19:227-230.
- Ishimatsu J, Yoshimura O, Tetsuou M, Hamada T. Evaluation of an aneurysm of the vein of Galen in utero by pulsed and color doppler imaging. Am J Obstet Gynecol 1991;164:743-744.
- Yamashita Y, Abe T, Ohara N et.al. Successful treatment of neonatal aneurysmal dilatation of the vein of Galen: the role of prenatal diagnosis and trans-arterial embolization. Neuroradiology 1992;34:457-459.
- Ordorica SA, Marks F, Frieden FJ et.al. Aneurysm of the vein of Galen: a new cause for Ballantyne syndrome. Am J Obstet Gynecol 1990;162:1166-1167.
- Reiter A, Huhta J, Carpenter R et.al. Prenatal diagnosis of arteriovenous malformation of the vein of Galen. J Clin Ultrasound 1986;14:623-628.
- Comstock C, Kirk J. Arteriovenous malformations. J Clin Med 1991;10:361-365.
- Ballester MJ, Raga F, Serra-Serra V, Bonilla-Musoles F. Early prenatal diagnosis of an ominous aneurysm of the vein of Galen by color doppler ultrasound. Acta Obstet Gynecol Scand 1994;73:592-595.
- Worswick L, Lamont R, Thomas R, Gordon H. Prenatal ultrasonic diagnosis of an aneurysm of the vein of Galen. Br J Radiol 1992;65:609-610.
- Rodesch
G, Hui F, Alvarez H et.al.
Prognosis of antenatally diagnosed vein of Galen
aneurysmal malformation. Child's Nerv Syst 1994;10:79-83.