|
ZELLWEGER’S
SYNDROME |
- This is a lethal condition which has a birth prevalence of 1:25000.
- Autosomal recessive.
- Seven PEX genes have been found associated with this condition (PEX 1, 2, 5, 7, 10, 12 and 16) (3). Prenatal diagnosis is available by assessment of peroxisomal beta-oxidation activity or by mutation analysis when the mutation is known (4).
- It is a protype of the group of perixisome-deficiency disorders. Peroxisomes are small cellular organelles containing multiple compounds that are essential for normal growth and development. Biochemical functions that occur within peroxisomes include beta oxidation of fatty acids, alpha oxidation of phytanic acid and biosynthesis of cholesterol. Peroxisomal disorders are classified into three groups (2):
Group A: Deficiency of peroxisomes with generalized loss of peroxisomal function – Zellwegers syndrome, neonatal adrenoleukodystrophy,
infantile Refusum disease.
Group B: Loss of multiple peroxisome functions (peroxisomes present) – Rhizomelic chondrodysplasia punctata, Zellwegerlike syndrome.
Group C: Loss of single peroxisome function (peroxisomes present) – X-linked adrenoleukodystrophy and variants, Acyl-CoA oxidase deficiency,
Bifunctional enzyme and Peroxisomal thiolase deficiency and other rare deficiencies.
- It is characterized by absence or marked decrease in peroxisomes resulting in profound muscular hypotonia.
- Death occurs in the first two years of life, usually due to chest infection and liver failure.
|
|
|
|
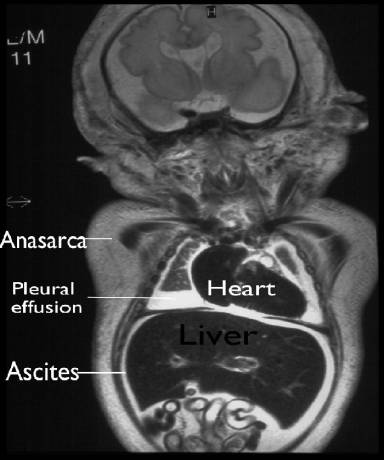
MR Coronal View |
|
|
MR Sagittal View |
|
|
MR demonstrating cystic hygromas |
|
|
Post-natal Xray pelvis |
|
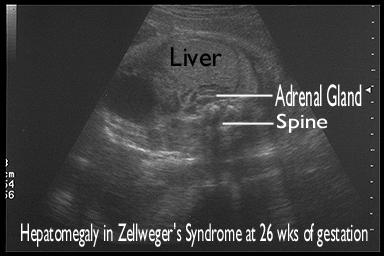
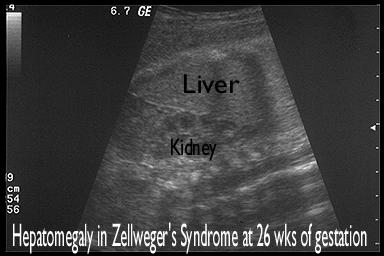
Hepatomegaly
at 26 weeks of gestation |
|
|
|
|



REFERENCES |
- Bilardo CM, Pajkrt E,
de Graff IM et.al. Outcome of fetuses with enlarged nuchal translucency
and normal karyotype. Ultrasound Obstet Gynecol 1998;11:401-406.
- Barkovich
AJ, Peck WW. MR of Zellweger syndrome. AJNR 1997;18:1163-1170.
- Honsho
M, Tamura S, Shimozawa N, Suzuki Y, Kondo N, Fujiki Y. Mutation in PEX 16
is causal in the peroxisome-deficient Zellweger syndrome of
complementation group D. Am J Hum Genet 1998; 63: 1622-1630
- Moser
AE, Singh I, Brown FR 3rd, Solish GI, Kelley RI, Benke PJ, Moser HW. The
cerebrohepatorenal (Zellweger) syndrome. Increased levels and impaired
degradation of very-long-chain fatty acids and their use in prenatal
diagnosis. N Engl J Med 1984; 310: 1141-1146