|
ENLARGED /
MEGA-CISTERNA MAGNA BLAKE’S POUCH
CYST |
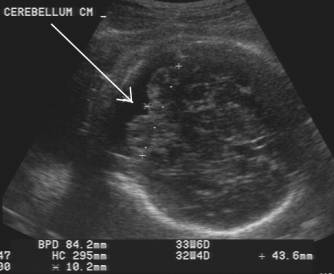
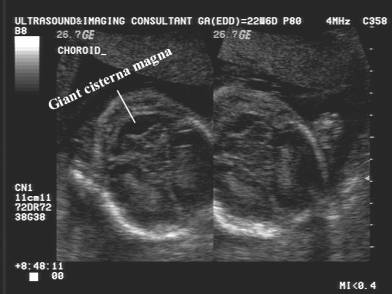
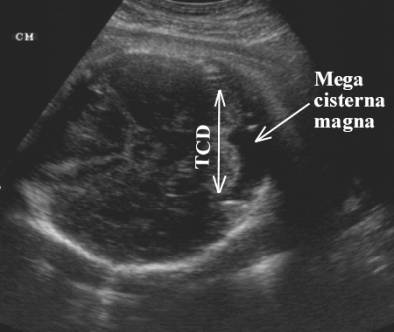
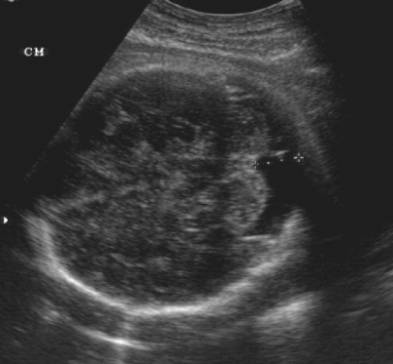
- Cisterna magna enlarged - >10mm. Free communication with perimedullary subarachnoid space. The cisterna may be so large that it extends laterally, posteriorly and superiorly far beyond the normal anatomic limits of the cisterna magna. The cisterna may also extend superiorly through a posterior dehiscence of the tentorium cerebelli .
|
|
|

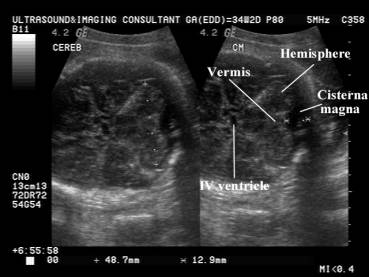
- Cerebellar vermis - intact and normal.
- Fourth ventricle -
- Cerebellum -
- Ventriculomegaly - unusual.
- A subarachnoid septa / dural fold is usually seen within the cistern.
- It may extend to various degrees behind the vermis and at times even above it.
- The tentorium cerebelli are normally located.
- The occipital bone may be scalloped and remodeled by the CSF pulsations.
|
Large cisterna
magna Normal dural fold within cisterna magna Normal
cerebellum and trans-cerebellar diameter Normal fourth
ventricle |
|
|
|
|

ETIOLOGY |
· Normal variation - isolated mega cisterna magna is thought to be an anatomic variant with no clinical significance (12). Bodensteiner et al. (13) found that isolated mega cisterna magna may be a marker for abnormal brain function most likely due to subtle disturbances in brain development.
· Cerebellar hypoplasia - Cerebellar hypoplasia is often associated with trisomies 13, 18 and 21 (14).
· Communicating hydrocephalus,
· The high incidence of mega cisterna magna is closely related to cerebellar hypoplasia.
|
|
|
|
|
|
|
|
|


ASSOCIATION WITH CHROMOSOMAL ANOMALIES |
|
Reference |
n |
Karyotyping
|
Cisterna
magna |
GA
at diagnosis |
|
1 |
5 |
Trisomy 18 |
Enlarged |
32-36.5 |
|
2 |
15 |
|
Enlarged |
14-38 |
|
|
18 |
Karyotypic anbormality |
|
|
|
|
·
12
-Trisomy 18 |
Enlarged |
26-36 |
|
|
|
·
3 -
Trisomy 13 |
Enlarged |
20-31 |
|
|
|
·
1 -
46,XX t(21q) |
Enlarged |
22 |
|
|
|
·
1 -
46,XY |
Enlarged |
28 |
|
|
|
·
1 -
45,X |
Enlarged |
20 |
|
|
3 |
20 |
Trisomy 18 |
Enlarged |
14.7-34.3 |
|
4 |
6 |
Trisomy 18 |
Enlarged |
Third trimester |
|
5 |
1 |
Partial trisomy 9 & 21 |
Enlarged |
24 |
|
6 |
1 |
Trisomy 21 |
Enlarged |
24 |
Some authors have reported that measurement of cisterna magna is a poor screening test for the detection of abnormal fetal karyotypes (7,8).
· Haimovici et al. (9) reviewed all the sonograms of 15 fetuses with isolated enlargement of the cisterna magna (> 10 mm) presenting in the third trimester. Normal pregnancy and neonatal outcome were observed in all cases.
- Watson et al. (10) reported that the cisterna magna measurement was normal in 28 fetuses with abnormal karyotypes.
|
# of cases |
Karyotype |
Size of cisterna magna |
GA of scan |
|
9 |
Trisomy 21 |
|
15-20 |
|
3 |
Trisomy 18 |
|
16-20 |
|
7 |
Sex chromosome
abnormalities |
|
14-20 |
|
8 |
Structural
chromosome abnormalities |
|
16-21 |
|
1 |
Triploidy |
|
15 |
- However, Nyberg et al. (11) found that the incidence of chromosomal abnormalities increases when an enlarged cisterna magna is found in association with other structural abnormalities. In reference 6, a dilated umbilical vein was also found, in addition to cisterna magna enlargement. Fetal karyotyping confirmed the diagnosis of trisomy 21. The implication of these findings is that if an enlarged cisterna magna combined with other ultrasound-diagnosed abnormalities is discovered, fetal karyotyping should be performed to look for chromosomal abnormalities.
PSEUDO MEGA CISTERNA MAGNA ORDANDY-WALKER
VARIANT (1) |
Increasing the transducer angle when examining
the posterior fossa can create this potential source of error. Scanning
in a semicoronal plane that was inferior and angled
in a more coronal plane may create this.
|
BLAKE’S
POUCH CYST |
Blake’s pouch cyst represents a posterior ballooning of the inferior medullary velum into the cisterna magna. It is recognized as a fluid collection inferior and posterior to the vermis.
- The fourth ventricle communicated with the cyst, but the cyst does not communicate with the basal subarachnoid space in the midline posteriorly.
- The vermis is completely or nearly completely formed, but thyere is mass effect on it which displaces it superiorly and anteriorly.
- The tentorium is usually elevated. (15).
REFERENCES |
1. Thurmond AS, Nelson DW, Lowensohn RI, Young WP, Davis L. Enlarged cisterna magna in trisomy 18: prenatal ultrasonographic diagnosis. Am J Obstet Gynecol 1989; 161: 83-5
2. Nyberg DA, Mahony BS, Hegge FN, Hickok D, Luthy DA, Kapur DR. Enlarged cisterna magna and the Dandy-Walker malformation: Factors associated with chromosome abnormalities. Obstet Gynecol 1991; 77: 436-42
3.
Steiger RM, Porto M,
4. Chen CP, Hung TH, Jan SW, Jeng CJ. Enlarged cisterna magna in the third trimester as a clue to fetal trisomy 18. Fetal Diagn Ther 1998; 13: 29-34
5. Chen CP, Shih JC. Prenatal diagnosis of bilateral ventriculomegaly and an enlarged cisterna magna in a fetus with partial 9 and partial trisomy 21. Prenat Diagn 1999; 19: 1175-80
6. Lai T -H Cheng Y –M, Chang F –M. Prenatal diagnosis of trisomy 21 in a fetus with an enlarged cisterna magna. Ultrasound Obstet Gynecol 2002;20:413-416.
7. Rosati P, Guariglia L. Transvaginal sonographic measurement of cisterna magna in fetuses with abnormal karyotype. Fetal Diagn Ther 1996; 11: 260-3
8. Mahony BS, Callen PW, Filly RA, Hoddick RA. The fetal cisterna magna. Radiology 1984; 153: 773-6
9. Haimovici JA, Doubilet PM, Benson CB, Frates MC. Clinical significance of isolated enlargement of the cisterna magna (> 10 mm) on prenatal sonography. J Ultrasound Med 1997; 16: 731-4
10. Watson WJ, Katz VL, Chescheir NC, Miller RC, Menard MK, Hansen WF. The cisterna magna in second-trimester fetuses with abnormal karyotypes. Obstet Gynecol 1992; 79: 723-5
11. Nyberg DA, Kramer D, Resta RG, Kapur R, Mohony BS. Prenatal sonographic findings of trisomy 18. Review of 47 cases. J Ultrasound Med 1993; 2: 103-13
12. Ieshima A, Kisa T, Yoshino K, Takashima S, Takeshita K. A morphometric CT study of Down's syndrome showing small posterior fossa and calcification of basal ganglia. Neuroradiology 1984; 26: 493-8
13. Bodensteiner JB, Gay CT, Marks WA, Hamza M, Schaefer GB. Mega cisterna magna: a marker for maldevelopment of the brain? Pediatr Neurol 1988; 4: 284-6
14. Comstock CH, Boal DB. Enlarged fetal cisterna magna: appearance and significance. Obstet Gynecol 1985; 66: 25S-28S
15.
Calabro F, Arcuri F, Jinkins JR.
Blake’s pouch cyst. An entity within the Dandy Walker continuum. Neuroradiology 2000;42:290-295.