|
BORDERLINE VENTRICULOMEGALY |
Atrial
width above 15 mm from 14-16 weeks onward is usually associated with a poor
prognosis (1).
- 60% of the cases with
ventricular width
 15 mm had
associated structural malformations of the CNS and/or other organs.
15 mm had
associated structural malformations of the CNS and/or other organs. - In the study by Gaglioti et al pregnancy was terminated in most cases
diagnosed before 24 weeks (88%) and there was one case of spontaneous
miscarriage. Of the 60 fetuses with severe ventriculomegaly, only 10 (16%)
were alive and normally developed at the age of at least 2 years. Even
when the analysis was limited to cases of isolated ventriculomegaly, the
rate of normal neurodevelopmental outcome was
62.5%.
- Graham et al (7)
found major neurological morbidity at pediatric follow-up in 33% (3/9) of
survivors with isolated severe ventriculomegaly.
- Gaglioti
et al only diagnosed a relatively small percentage of cases (57%) before
24 weeks of gestational age (almost half of severe ventricular dilatations
developed later in prenatal life).
The
large variation in the frequency of associated anomalies reported in the
literature on borderline ventriculomegaly (2,3,5,6,9,10).
ranging from 10% (6) to 76% (2), might be due to
variation in the proportion of cases with mild and moderate ventriculomegaly;
unfortunately, in most studies data were not separately analyzed for cases with
atrial width < 12 mm or > 12 mm.
Only
Vergani et al (5) found that an atrial width
< 12 mm was associated with other anomalies in 6% of the cases, compared
with 56% when the atrial width was above 12 mm.
Gaglioti et al
reviewed 116 such cases. They separately analyzed cases of mild (10 to 12 mm)
and moderate (12.1 to 14.9 mm) ventriculomegaly and found that the latter ones
were significantly more often associated with structural anomalies (75%) than
mild cases (41%).
CLASSIFICATION |
<
10mm – normal
10-12
mm – borderline ventriculomegaly
>12
but <15 mm – mild
>15
mm – marked ventriculomegaly
ULTRASOUND |
- Look for structural
malformations.
- The risk of chromosomal anomalies
reported in the literature in these cases ranges from 0 to 14% (2-4,7, 9,10, 12,13).
- Screening for infections
(usually TORCH) is recommended when ventriculomegaly is diagnosed (5,6,8,14).
|
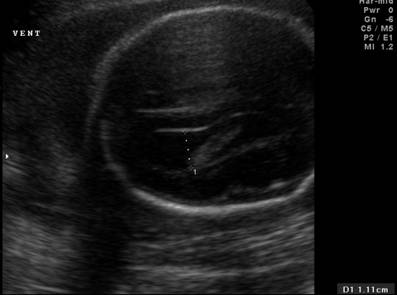
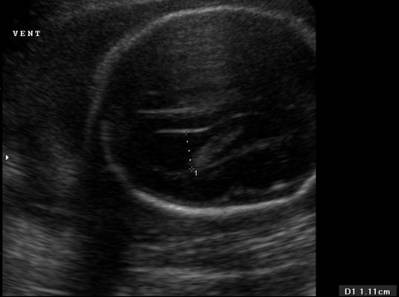
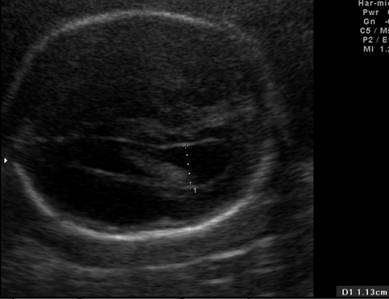
Far field ventricle |
Near field ventricle |
|
|
|
|
Ventricular atrium – 1.11 cm |
Ventricular atrium – 1.13 cm |
|
|
|

OUTCOME |
The
overall outcome was better when the ventriculomegaly was mild: it was normal in
93% of the cases compared with 75% in moderate cases.
Vergani et
al (5) reported similar results in isolated cases: a significantly lower
rate of developmental delay when atrial width was < 12 mm (3%) than when it
was 12-15 mm (23%).
Pilu et al
(6), in a review of the literature on 141 cases, reported a 3.8% rate of
abnormal neurodevelopmental outcome when the atrial
width was < 12 mm, compared to 14% when it was 12-15 mm.
Signorelli et
al (11) published results in 60
cases of mild isolated ventriculomegaly ![]() 12 mm,
reporting normal neurodevelopmental outcome in 100%
of the cases. They suggested considering this atrial width a variant of the
norm, once structural and chromosomal anomalies have been excluded.
12 mm,
reporting normal neurodevelopmental outcome in 100%
of the cases. They suggested considering this atrial width a variant of the
norm, once structural and chromosomal anomalies have been excluded.
REFERENCES
|
- Romero R , Pilu G , Jeanty P , Ghidini A , Hobbins JC (eds). The
central nervous system. In Prenatal
Diagnosis of Congenital Anomalies. Appleton & Lange:
- Goldstein RB, La Pidus AS, Filly RA, Cardoza J. Mild lateral cerebral ventricular dilatation in utero: clinical significance and prognosis. Radiology 1990; 176: 237-242
- Bromley B, Frigoletto FD Jr, Benacerraf BR. Mild fetal lateral ventriculomegaly: clinical course and outcome. Am J Obstet Gynecol 1991; 164: 863-867
- Bloom SL, Bloom DD, DellaNebbia C, Martin LB, Lucas MJ, Twickler DM. The developmental outcome of children with antenatal mild isolated ventriculomegaly. Obstet Gynecol 1997; 90: 93-97.
- Vergani P, Locatelli A, Strobelt N, Cavallone M, Ceruti P, Paterlini G, Ghidini A. Clinical outcome of mild fetal ventriculomegaly. Am J Obstet Gynecol 1998; 178: 218-222
- Pilu G, Falco P, Gabrielli S, Perolo A, Sandri F, Bovicelli L. The clinical significance of fetal isolated cerebral borderline ventriculomegaly: report of 31 cases and review of the literature. Ultrasound Obstet Gynecol 1999; 14: 320-326.
- Graham E, Duhl A, Ural S, Allen M, Blakemore K, Witter F. The degree of antenatal ventriculomegaly is related to pediatric neurological morbidity. J Matern Fetal Med 2001; 10: 258-263
- den Hollander NS, Vinkesteijn A, Schmitz-van Splunder P, Catsman-Berrevoets CE, Wladimiroff JW. Prenatally diagnosed fetal ventriculomegaly: prognosis and outcome. Prenat Diagn 1998; 18: 557-566.
- Mercier A, Eurin D, Mercier PY, Verspyck E, Marpeau L, Marret S. Isolated mild fetal cerebral ventriculomegaly: a retrospective analysis of 26 cases. Prenat Diagn 2001; 21: 589-595.
- Patel MD, Filly
- Signorelli M, Tiberti A, Valseriati D, Molin E, Cerri V, Groli C, Bianchi UA. Width of the fetal lateral ventricular atrium between 10 and 12 mm: a simple variation of the norm? Ultrasound Obstet Gynecol 2004; 23: 14-18
- Tomlinson MW, Treadwell MC, Bottoms SF. Isolated mild ventriculomegaly: associated karyotypic abnormalities and in utero observations. J Matern Fetal Med 1997; 6: 241-244
- Terry M, Calhoun BC, Walker W, Apodaca C, Martin L, Pierce B, Hume RF, Evans MI. Aneuploidy and isolated mild ventriculomegaly. Attributable risk for isolated fetal marker. Fetal Diagn Ther 2000; 15: 331-334.
- Pilu G, Hobbins JC. Sonography of fetal cerebrospinal anomalies. Prenat Diagn 2002; 22: 321-330