|
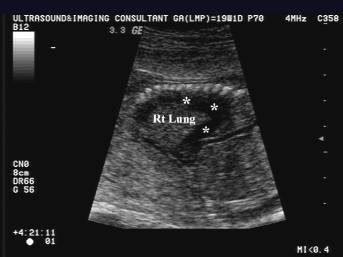
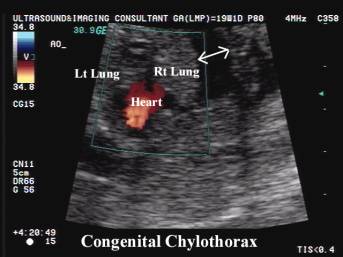
CONGENITAL
CHYLOTHORAX |
During embryonic development bilateral thoracic channels exist. The upper third of the right duct and lower two thirds of the left duct obliterate producing multiple cross channels draining into the permanent thoracic duct. Because of this anatomic arrangement leakage from the lower portion of the duct produces a left pleural effusion.
· 1:10,000 births.
·
Overall mortality 25% (1-3).
ULTRASOUND |
- Unilateral effusion (90%) > bilateral fluid collections.
- Right side more commonly affected than the left side.
- Males are affected twice as often as females (4).
- Fetal age of presentation ranges from 19 weeks to term.
- Polyhydramnios may occur due to compression of the fetal esophagus, SVC or heart by the effusion (4,5).
- Prenatal diagnosis is difficult as the fluid is clear and colorless because of the absence of chylomicrons. The classic chylous appearance is evident once oral milk feeding has begun. Lipoprotein electrophoresis of pleural fluid from the fetus may show typical predominance of high-density lipoprotein allowing a confident diagnosis of chylothorax.
|
|
|
|
|
|
|
|
|
|
|
|





ASSOCIATIONS |
- Isolated (8).
- Trisomy 21 (associated with 4.9% of isolates pleural effusions) (1,2,6,7).
- Tracheo-esophageal fistula.
- Extralobar bronchopulmonary sequestration.
COMPLICATIONS |
- Pulmonary hypoplasia (due to compression).
- Fetal hydrops (disruption of venous return).
- Congestive heart failure.
REFERENCES |
- Reece EA, Goldstein I, Hobbins JC. Fundamental of Obstetric and Gynecologic Ultrasound, 1994.
- Callen PW. Ultrasonography in Obstetrica and Gynecology (3rd edition), 1994.
- Dendale J, Comet P, Amram D et.al. Prenatal diagnosis of chylothorax. Arch Pediatr 1999;6:867-871.
- Randolph JG, Gross RE. Congenital chylothorax. Arch Surg 1957;74:405-419.
- Petres RE, Redwine FO, Cruikshank DP. Congenital bilateral chylothorax: Antepartum diagnosis and successful intrauterine surgical management. JAMA 1982;248:1360-1361.
- Echeverria LJ, Benito A, Arena AJ et.al. Quilotorax congenito. An Esp Pediatr 1998;49:161-164
- Hagay Z, Reece A, Roberts A et.al. Isolated foetal pleural effusion – a prenatal management dilemma. Obstet gynecol 1993;81:147-152.
- Brito T Olivera C Sousa L et.al. Congenital chylothorax: a case report. Ultrasound Obstet Gynecol 2002;20:70-71.