|
CHEST WALL MASSES |
CHEST WALL HAMARTOMA (1,2) |
- Echogenic mass with posterior shadowing suggesting calcification.
- Mass may extend into the thoracic cavity making it impossible to distinguish from a calcified thoracic neuroblastoma.
- Mass is extrapleural and affects one or more ribs.
- Ribs near center of mass is eroded or destroyed whereas the ribs near the periphery are deformed or eroded.
CYSTIC HYGROMA OF THE CHEST WALL AND AXILLA (3-5) |
- Multiseptate fluid-filled mass (resembles a cystic hygroma in other locations).
- 70-90% of postnatally diagnosed cystic hygromas are found in the neck, and about 20% are located in the axilla (2). Other locations have a prevalence of under 10% (3). Prenatal diagnosis of axillary cystic hygroma have been previously described (2-4).
- Link to
Ultrasound
LYMPHANGIECTASIA |
- Involves the chest wall in a similar fashion to cystic hygroma, but there is marked involvement of the subcutaneous tissue. This distinguishes lymphangiectasia from cystic hygroma and subcutaneous edema from fetal hydrops.
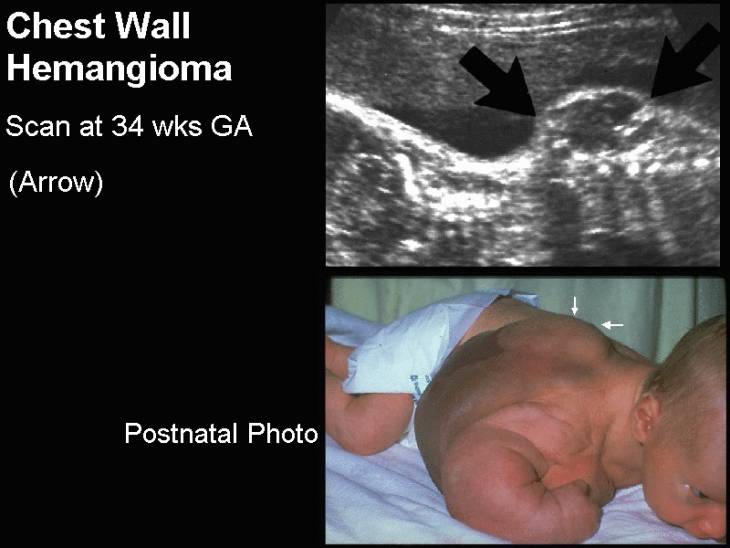
HEMANGIOMA |
- Found in Klippel-Trenaunay-Weber syndrome.
- May have thick septations and usually extend onto an extremity.
- Other rare masses such as melanoma would presumably be homogeneously solid.
|
|
REFERENCES |
- Brar MK, Cubberley DA, Baty BJ et.al. Chest wall hamartoma in a fetus. J Ultrasound Med 1988;7:217-220.
- Masuzaki H, Masuzaki M, Ishimaru T et.al. Chest wall hamartoma diagnosed prenatally using ultrasonography and computed tomography. J Clin Ultrasound 1996;24:83-85.
- Reichler A, Bronshtein M. Early prenatal diagnosis of axillary cystic hygroma. J Ultrasound Med 1995;14:581-584.
- Anderson NG, Kennedy JC. Prognosis in fetal cystic hygroma. Aust NZ J Obstet Gynecol 1992;32:36.
- Hoffman-Tretin J, Koenisberg M, Ziprowski M. Antenatal demonstration of axillary cystic hygroma. J Ultrasound Med 1994;7:233.