|
CONGENITAL LOBAR
EMPHYSEMA (CLE) |
Congenital lobar emphysema is a rare disorder characterized by air trapping in a segmental or lobar distribution, which causes local mass effect (1), but does not destroy the tissue. Postnatally, CLE is caused by air trapping of the obstructed bronchus. The obstruction results in a ball-valve mechanism which does not allow for deflation of the hyperinflated lung.
ETIOLOGY |
- Deficient cartilaginous support of the tracheobronchial tree.
- Abnormal supporting stroma of the alveolar cells.
- Intrinsic or extrinsic bronchial obstruction (2).
Intrinsic obstruction is either due to a defect in the bronchial wall or it’s cartilage, and less commonly due to an intraluminal lesion such as folds, webs or mucus plugs.
Extrinsic obstruction results from compression from teratomas,
CCAM, bronchogenic cysts, cardiac or vascular
abnormalities.
ULTRASOUND |
Workers (3,4) have found that CLE is as common as bronchopulmonary sequestration and almost as common as congenital cystic malformation, however it is rarely diagnosed antenatally (1). The reason for this may be based on fetal pulmonary physiology and the production of fluid by the lungs causes positive pressure on the fetal trachea and bronchi during apnea thus maintaining the patency of the relatively floppy conductive airways of the fetus with CLE (5).
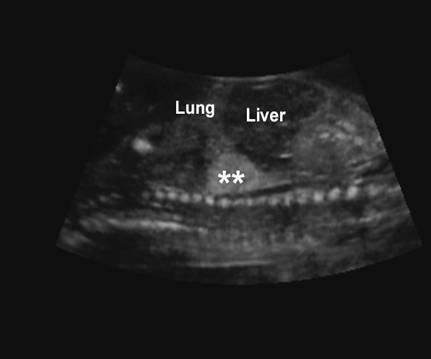
· Large echogenic chest mass (this is usually only evident during the canalicular period i.e. 17-24 weeks of gestation once the alveoli have formed). The explanation for this could be found in the stage of lung development present. In the pseudoglandular period of 8-16 weeks, conducting airways to the level of the terminal bronchioles are developing as well as bronchial glands and goblet cells. This development is completed by week 16. Saccules, which consist of respiratory bronchioles, alveoli ducts and alveoli, are formed during the canalicular period of 17-24 weeks (7). It is possible that even though lung fluid is being produced from week 10 onwards (7), not enough is produced until the canalicular period of 17-24 weeks to over-distend the lungs, making them echogenic. As CLE is the over-distension of alveoli, and these do not form until the canalicular period, echogenic lungs from CLE would not be expected before this gestation.
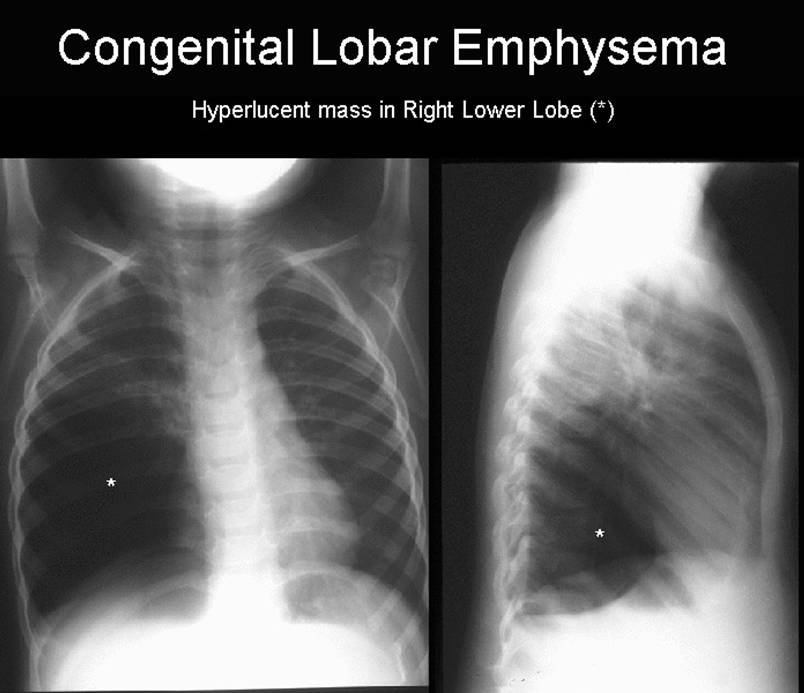
· Middle and upper lobes are most commonly involved. A single report of lower lobe involvement has been reported (6).
· Mediastinal shift.
· Depression of the hemidiaphragm.
· Polyhydramnios.
· Ascites.
|
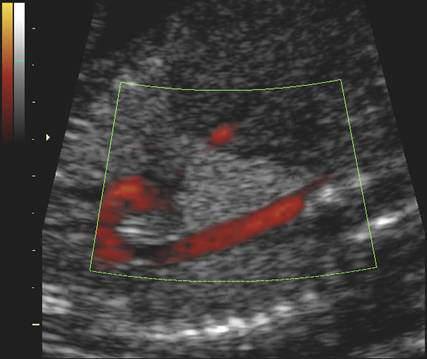
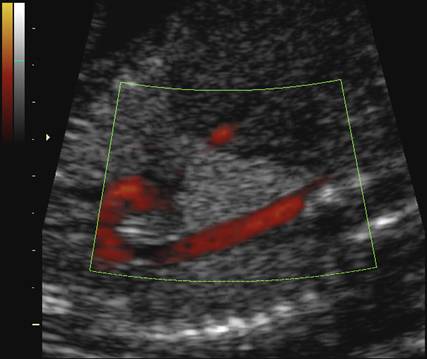
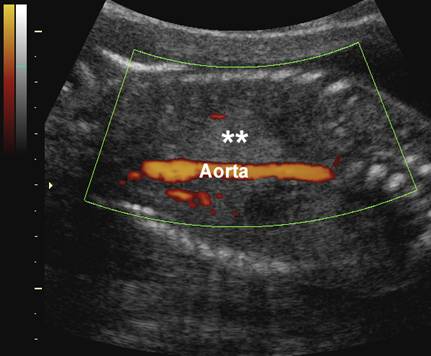
Echogenic
right lung mass with no vascular supply from the thoracic aorta – 21 weeks
GA |
|
|
|
|
|
|
|
|
|
|
|
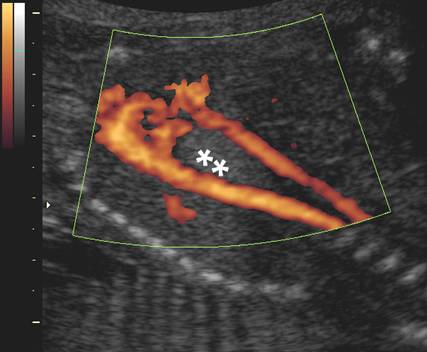
Spontaneous
resolution of lung mass by 32 weeks of gestation |
|
|
|
|
|
|
|

PROGNOSIS |
Review
of the mortality and morbidity rates in two infant series (10 infants in one
series and six in another) revealed no deaths in children diagnosed and
surgically treated for CLE (3,8). Prognosis and survival with surgery is good
(8-10). The infants in the three antenatal cases reported all survived after lobectomy (1,16). In general the
spontaneous disappearance of fetal lung echogenicity
is usually associated with a good outcome (1, 12-15). The advantage of
antenatal detection is in pediatric follow up after birth, which allows early
diagnosis and management before the infant becomes symptomatic, as shown in
this case
REFERENCES |
- Richards DS, Langham MR, Dolson LH. Antenatal presentation of a child with congenital lobar emphysema. J Ultrasound Med 1992;11:165-168.
- Raynor AC, Capp MP, Sealy WC. Lobar emphysema of infancy. Ann Thorac Surg 1967;4:374.
- Bailey PV, Tracy T, Connors RH et.al. Congenital bronchopulmonary malformations. J Thoracic Cardiovasc Surg 1990;99:597.
- Haller JA, Golladay ES, Pickard LR et.al. Surgical management of lung bud anomalies; Lobar emphysema, bronchogenic cyst, cystic adenomatoid malformation, and intralobar pulmonary sequestration. Ann Thorac Surg 1979;28:33.
- Alcorn D, Adamson TM,
Lambert TF et.al. Morphological effects of
chronic tracheal ligation and drainage in the
fetal lamb lung. J Anat 1977;123:649.
- Quinton AE, Smoleniec JS. Congenital lobar emphysema – the disappearing chest mass: antenatal ultrasound appearance. Ultrasound Obstet Gynecol 2001;17:169-171.
- Swischuk LE. Acute respiratory distress in a young infant. Pediatric Emergency Care 1991; 7: 255-257
- Schwartz MZ & Ramachandran
P. Congenital malformations of the lung and mediastinum
 a
quarter century of experience from a single institution. J Pediatric Surg
1997; 32: 44-47
a
quarter century of experience from a single institution. J Pediatric Surg
1997; 32: 44-47 - Al-Bassam A, Al-Rabeeah A, Al-Nassar S et al. Congenital cystic disease of the lung in infants and children (experience with 57 cases). Eur J Paediatric Surg 1999; 9: 364-368
- Takeda S, Miyoshi S, Inoue M et al. Clinical spectrum of congenital cystic disease of the lung in children. European J Cardio-Thoracic Surg 1999; 15: 117-118
- Richards DS, Langham MR, Dolson LH. Antenatal presentation of a child with congenital lobar emphysema. J Ultrasound Med 1992; 11: 165-168
- Langer B, Donato L, Riethmuller C, Becmeur F, Dreyfus M, Favre R, Schlaeder G. Spontaneous regression of fetal pulmonary sequestration. Ultrasound Obstet Gynecol 1995; 6: 33-39
- Roelofsen J, Oostendorp R, Volovics A, Hoogland H. Prenatal diagnosis and fetal outcome of cystic adenomatoid malformation of the lung: case report and historical survey. Ultrasound Obstet Gynecol 1994; 4: 78-82
- Achiron R, Strauss S, Seidman DS, Lipitz S, Mashiach S, Goldman B. Fetal lung hyperechogenicity: prenatal ultrasonographic diagnosis, natural history and neonatal outcome. Ultrasound Obstet Gynecol 1995; 6: 40-42
- Sepulveda W &
- Carrol ED,