|
ULTRASOUND OF
VENTRICULAR SEPTAL DEFECTS |
The best view for diagnosing VSD's is the subcostal four-chamber view as the ultrasound beam is perpendicular to the interventricular septum (axial resolution is better than lateral resolution). Other important views include the left and right ventricular outflow tract views and the short axis views of the ventricles.
THE
|
PITFALL IN
THE DIAGNOSIS OF VSD’S
|
- Hypoechoic dropout if the septum is parallel to the ultrasound beam
- Small defects may be missed as resolution limits detection to 2mm.
|
Pitfall in the
diagnosis of VSD’s on apical four chamber
view Note the small striations seen in the septum on the gray-scale and color images do not represent defects in the septum. These striations are not seen on the subcostal views. |
|
|
|
|
Pseudo-VSD
Pseudo defect in the membranous septum in the apical four
chamber view. No defect was seen in the subcostal
view. |
|
|
|
|


ULTRASOUND
IN VENTRICULAR SEPTAL DEFECTS
|
- Isolated or complex (associated with other complex cardiac defects)
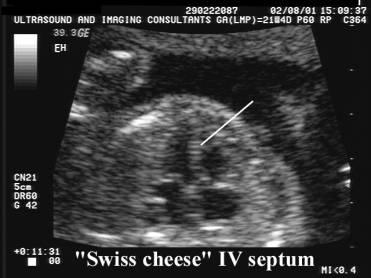
- Single or multiple defects.
- Perimembranous (73%), muscular (37%) at our institute.
|
|
Video clip of a
VSD - high muscular defect Video clip of a
VSD - mid muscular defect Video clip of a
VSD – low apical defect
|
|
|
|
|
|

GRAY
SCALE IMAGES
|
- Most are perimembranous and subaortic, however up to one third are not detected on gray-scale images of the four-chamber view (1,2).
|
|

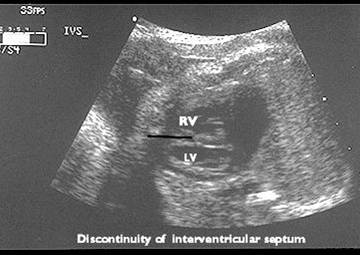
- An anechoic area in the septum (this finding must be confirmed in more than one sonographic plane to exclude hypoechoic dropout)
- Seen as an area of discontinuity in the interventricular septum. The T-sign represents an area of hypoechoic dropout bordered by the hyperechogenic, blunted edge of the intact portion of the septum.
- The T artifact was originally described in neonates and young adults as scattered reflections around the edges of a real VSD (6). The T artifact in the standard cardiac views has been reported to have a sensitivity of 88% and a specificity of 100% in the
detection of VSDs (6).
|
Area of
discontinuity in interventricular septum |
|
|
|
|
|
|
Area of discontinuity must not be appreciated on gray-scale images |
||
|
|
|
|




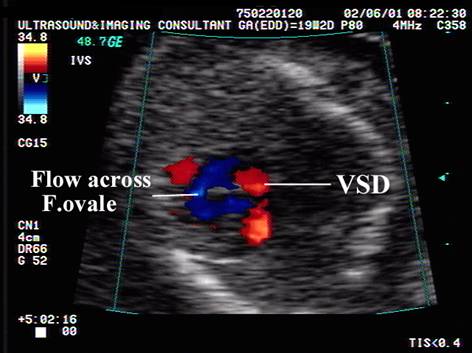
COLOR
DOPPLER IMAGES
|
- Color doppler vastly improves the accuracy of detection of small VSD's (3,4). The ventricular septum may look normal on conventional gray-scale images.
- Velocity of the shunt is usually low in isolated defects. If the velocity is high, it is important to exclude any cause of ventricular hypertension (outflow tract obstruction or disease of the atrio-ventricular valves).
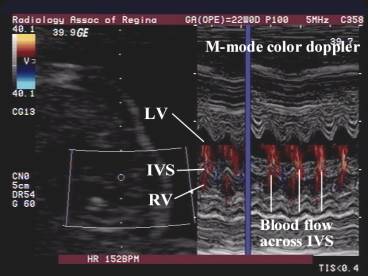
- M-mode color doppler across the VSD supplies information on the velocity and direction of the shunt.

- VSD's may be missed on color doppler due to equalization of pressures in the left and right ventricles (no flow across the defect (unlike pediatric patients where there is a pressure gradient).
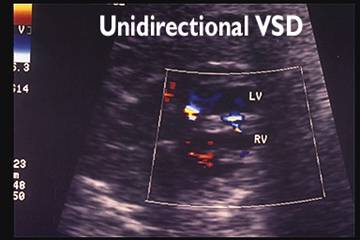
- Direction of the shunt:
- Bi-directional (left to right during systole and right to left during diastole). This appearance is not present in all patients and may vary with time).
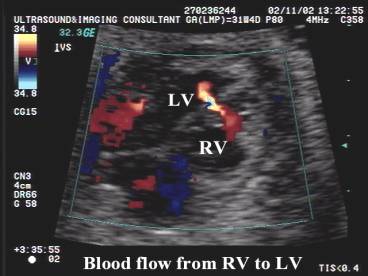
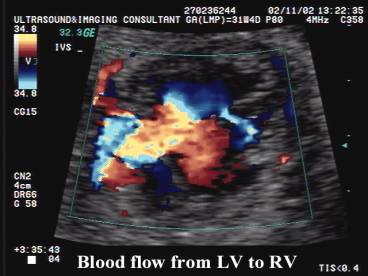
- Unidirectional (left to right shunting).


- High velocity jets are rare.
|
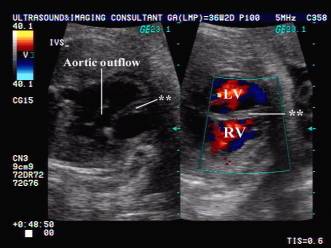
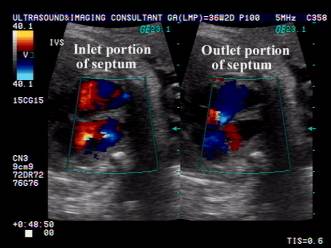
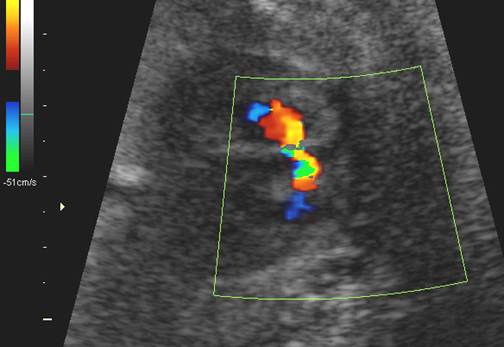
Types of VSD’s |
||
Membranous (perimembranous) VSD |
||
|
|
|
|
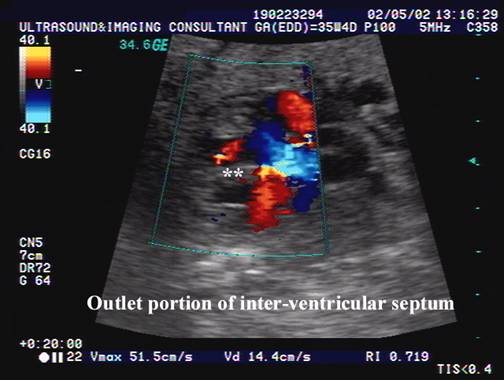
VSD – 4
mm outlet perimembranous VSD
|
||
|
|
|
|
|
||
|
|
|
|
|
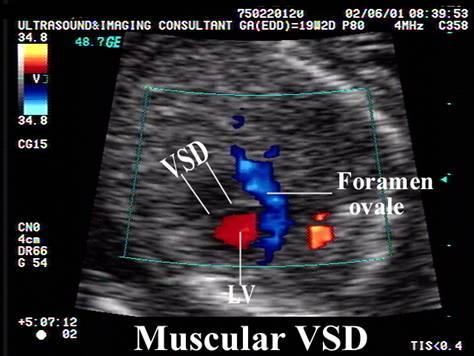
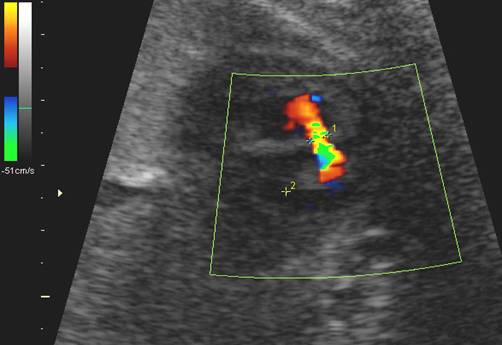
Muscular
defect at the level of the outlet |
||
|
|
||
|
|
||
|
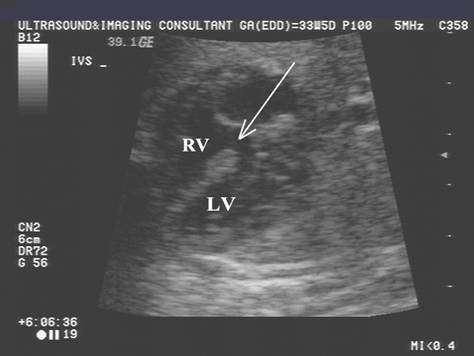
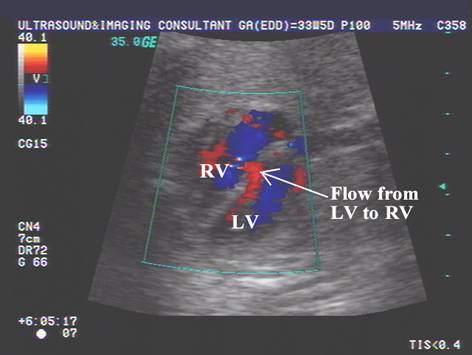
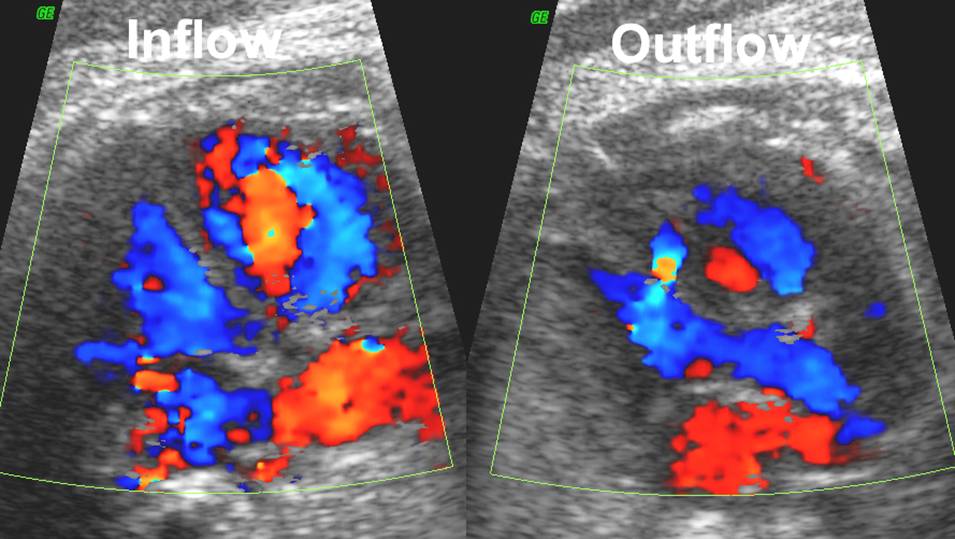
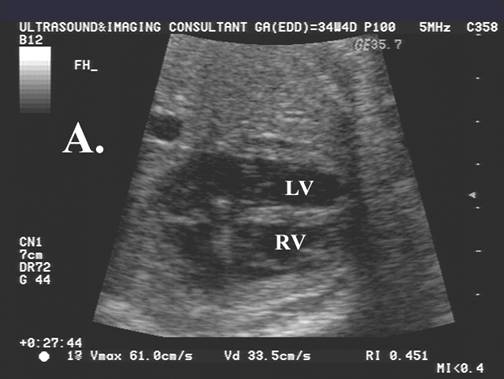
Apical VSD: ·
A,B. Non visualization of VSD on gray scale
images. ·
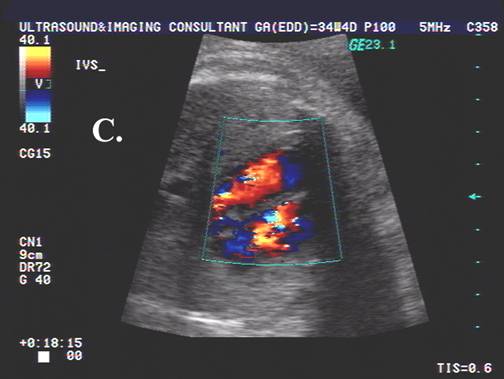
C. Apical portion
of ventricular septum obscured by rib
shadow. ·
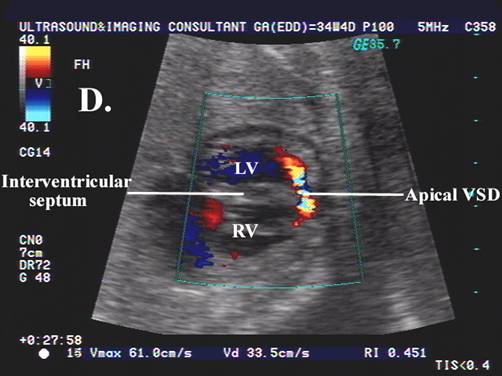
D, E, F. Color doppler images
demonstrating apical VSD (5mm) with
flow from RV to |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
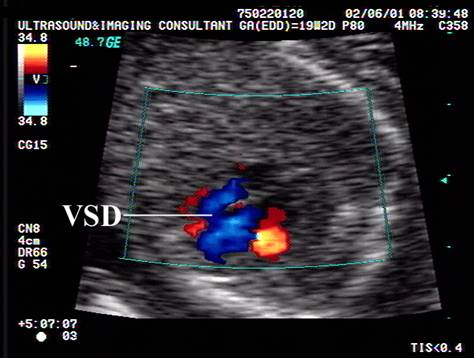
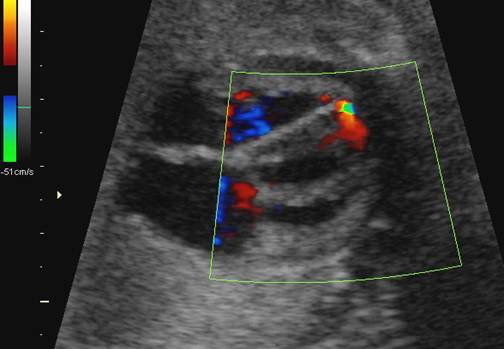
Inlet VSD: -
Bidirectional flow. -
Spontaneous post-natal closure at 3 months of age |
||
|
|
|
|
|
|
|
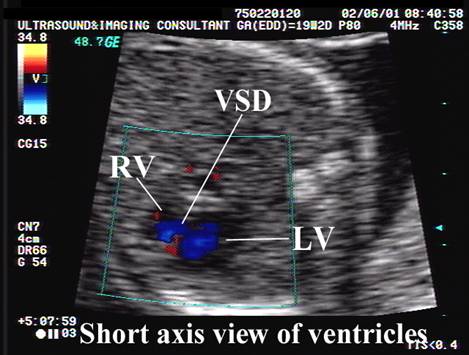
|
Short-axis view of Muscular VSD
|
||
|
|
|
|
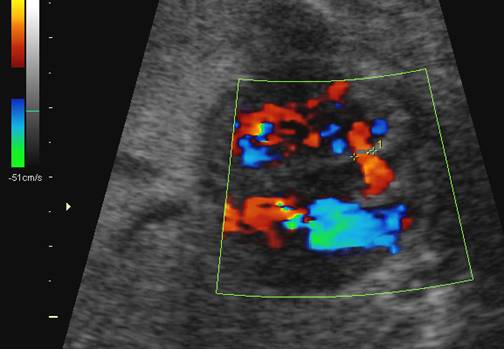
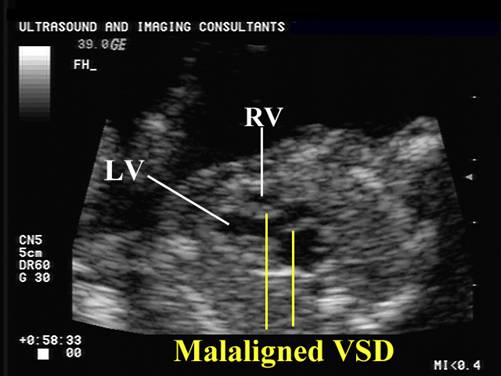
Malaligned VSD
·
Hypoplastic right
ventricle. ·
Malaligned VSD. ·
Tricuspid stenosis. |
||
|
|
|
|
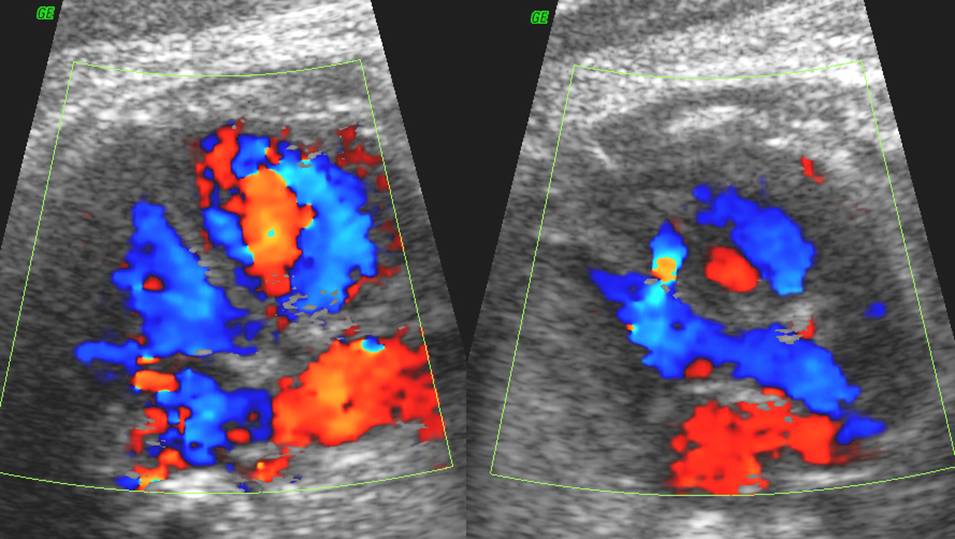
Single versus multiple VSD’s |
||
|
|
|
|









REFERENCES
|
- Copel JA, Pilu G, Green J et.al. Fetal echocardiographic screening for congenital heart disease: the importance of the four chamber view. Am J Obstet Gynecol 1987;157:648-655.
- Benacerraf BR, Prober RB, Sanders SP. Accuracy of fetal echocardiography. Radiology 1987;165:847-849.
- Sutherland GR, Smyllie JH,
- Crawford DC, Chita SK, Allan LD. Prenatal detection of congenital
heart disease: factors affecting obstetric management and survival. Am J Obstet Gynecol 1988;159:352-356.
- Canale
JM, Sahn DJ, Valdes-Cruz LM, Allen HD, Goldberg
SJ, Ovitt TW. Accuracy of two-dimensional
echocardiography in the detection of aneurysms of the ventricular septum. Am Heart J 1981; 101: 255-259