|
TRUNCUS ARTERIOSUS |
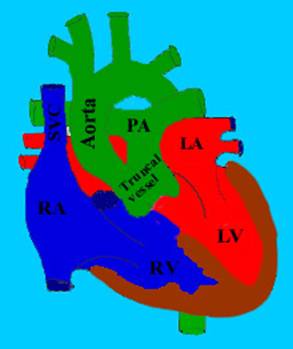
Truncus arteriosus is
characterized by a single large vessel arising from the base of the heart
supplying both systemic and pulmonary circulations as well as the coronary
arteries (1). It is often referred to as persistent truncus
arteriosus as the truncus
is a normal embryologic cardiac structure that is only anomalous if it persists
throughout cardiac development. 20-40% risk of 22q11.2 deletion.
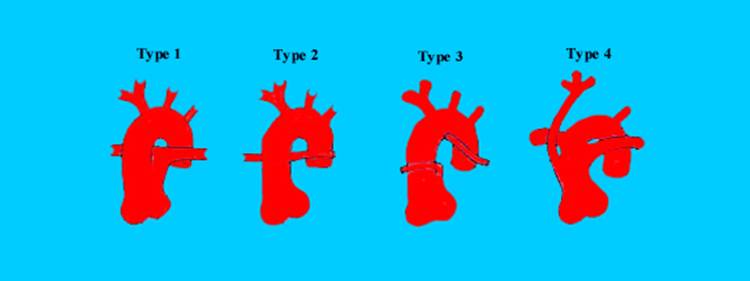
CLASSIFICATION (2,3) |
|
Type I |
- Pulmonary artery bifurcates into left and right branches after it arises from the ascending portion of the truncal vessel. |
||
|
Type II |
- Right and left pulmonary arteries arise separately from the posterior truncus. |
||
|
Type III |
Pulmonary arteries arise from the sides of the proximal truncus. Pulmonary arteries arise from
the sides of a single large truncal vessel (type
III) |
||
|
|
|
||
|
|
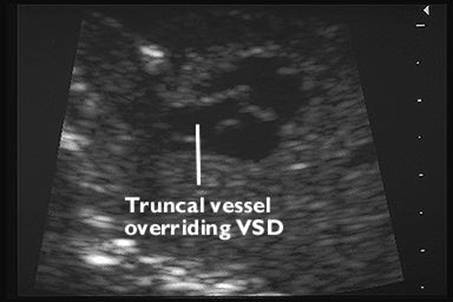
Single truncal
vessel overriding a large VSD |
||
|
|
|
||
|
Type IV |
- "Pseudotruncus" - absent pulmonary arteries |
||
|
Subtype A |
- Infundibular VSD present. |
||
|
Subtype B |
- VSD absent |
||
|
|
|
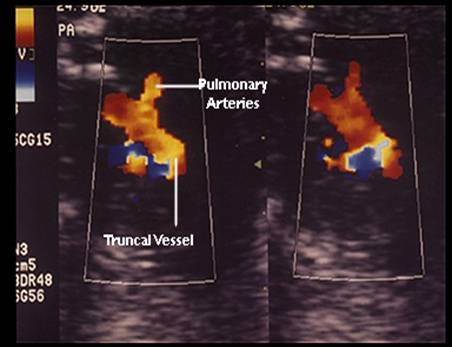
ULTRASOUND |
- Large truncal artery exiting the heart and:
- Overrides the ventricular septum.
- Receives blood from both the left and right ventricle.
- Supplies systemic, pulmonary and coronary circulations.
- Has the pulmonary arteries arising from the undivided truncus.
- The single arterial trunk
is larger than the normal aortic root and is connected to RV (42%),
- Truncal valve may have 2-6 cusps (2 cusps in 5%, 3 cusps in 60%, and four cusps in 25%), and may be incompetent in 10-15% of patients but is rarely stenotic.
- The semilunar valve is usually thickened, moves abnormally and overrides the VSD. Doppler studies may demonstrate incompetence of the valve.
- Direct continuity between one or two pulmonary arteries and the single arterial trunk.
- Large ventricular septal defect, which is malaligned.
- Absent ductus arteriosus in 50-75% of cases.
- Aortic anomalies (20%) including interruption of the aortic arch.
- Fetal hydrops may occur and is associated with a dismal outcome.
- Right sided aortic arch (15-30%).
- Non cardiac anomalies (48%).
DIFFERENTIAL DIAGNOSIS |
Differential Diagnosis of a Large Truncal Vessel Overriding a VSD
- Truncus arteriosus.
- Tetralogy of Fallot.
- Pulmonary atresia + VSD
REFERENCES |
- Allan LD,
- Collet RW, Edwards JE. Persistent truncus arteriosus. A classification according to anatomic types. Surg Clin North Am 1949;29:1245-1270.
- Van Praagh R, Van Praagh S. The anatomy of the common aorticopulmonary trunk and its embryologic implications. A Study of 57 necropsy cases. Am J Cardiol 1965;16:406-421.
- Hernanz-Schulman M, Fellows KE. Persistent truncus arteriosus: pathologic, diagnostic and therapeutical considerations. Semin Roentgenol 1985;20:121-129.