|
ULTRASOUND OF
EBSTEIN’S ANOMALY |
- Tricuspid valve
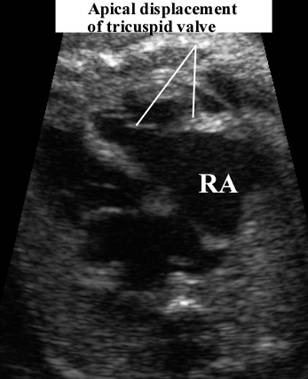
- Apical displacement of the septal leaflet. This is probably the most reliable diagnostic sign.
- Posterior leaflet usually displaced apically but the degree of displacement is variable.
- Anterior leaflet is not displaced and may be normal or large and redundant ("snail-like appearance").
- Small mobile parts of the leaflets lie deep in the RV.
- The above changes result in atrialization of the inflow portion of the RV (there may be little or no myocardium like Uhl's anomaly and functionally it behaves like the right atrium).
- Tricuspid incompetence may be present as only small parts of the valve cusps are free to move.
- Tricuspid dysplasia ranges from mild to severe, as the valve is either thickened or nodular.
- Tricuspid stenosis may result from thickened chordae and abnormal "linear" attachment between the valve cusps and trabeculae of the right ventricle, tethering the leaflet to the ventricular wall.
- Tricuspid atresia may be present in the most severe form (imperforate type of Ebstein's anomaly).
· Right atrium - usually massively enlarged.
· Right ventricle - usually dilated with a normal myocardium. RV dysplasia may occur (RV dilatation, decreased wall thickness and dyskinesia).
· Interventricular septum - The large RV may result in paradoxical motion of the interventricular septum.
This
may cause compression of the
· Fetal hydrops. +
· Arrhythmia - especially SVT.
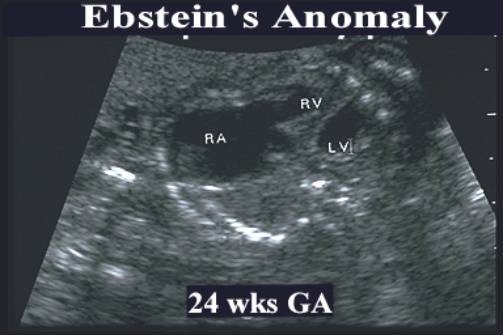
Ebstein’s Anomaly
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
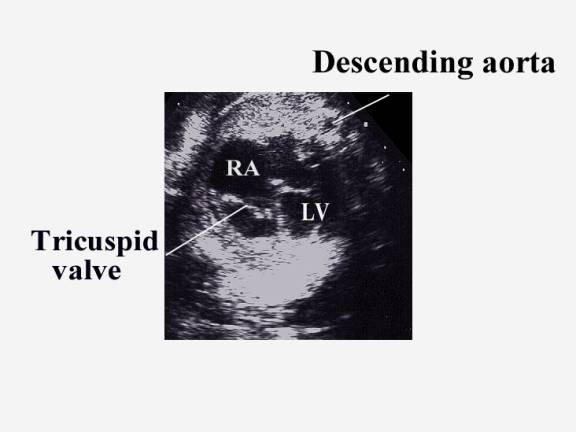
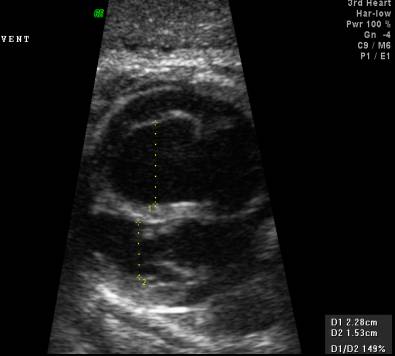
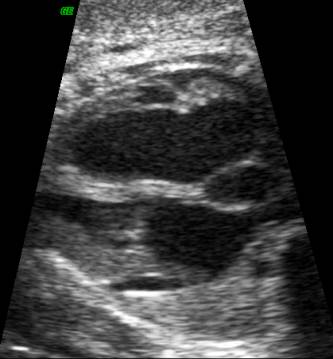
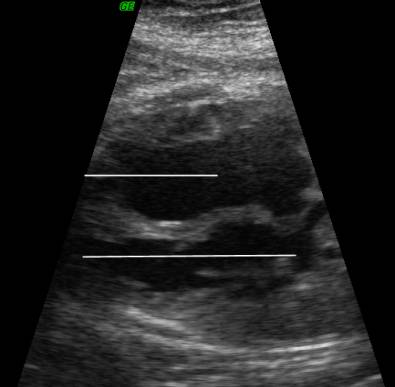
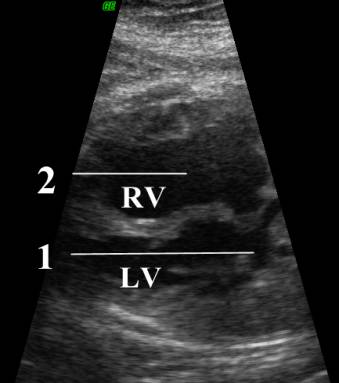
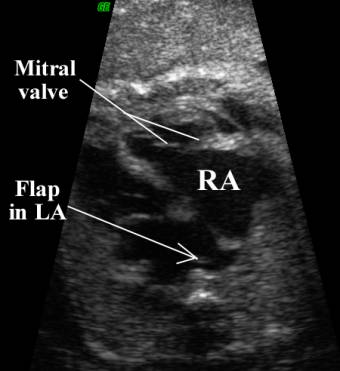
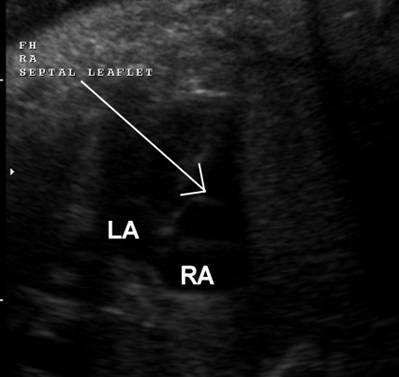
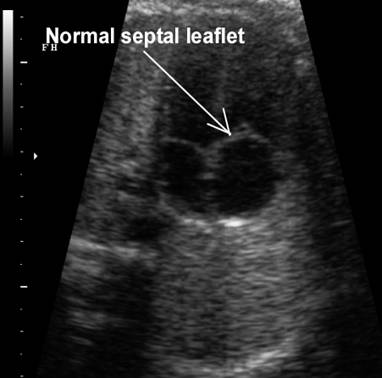
Tricuspid valve dysplasia demonstrates
apparent apical displacement of the septal leaflet. The bottom right image
demonstrates that the tricuspid valve leaflets are normally positioned and
not apically displaced, thus excluding Ebstein’s anomaly. |
|
|
|
|
DIFFERENTIAL DIAGNOSIS |
- Uhl's anomaly
- Tricuspid valve dysplasia. The valves are thickened and may be redundant or hypoplastic but attach normally in the atrioventricular groove (1). In Ebstein's anomaly the attaxhments of the septal and posterior leaflets are displaced to the right and the valve may be dysplastic. The distinction between the two conditions is based on the location of the valve (this may be difficult to determine antenatally).