|
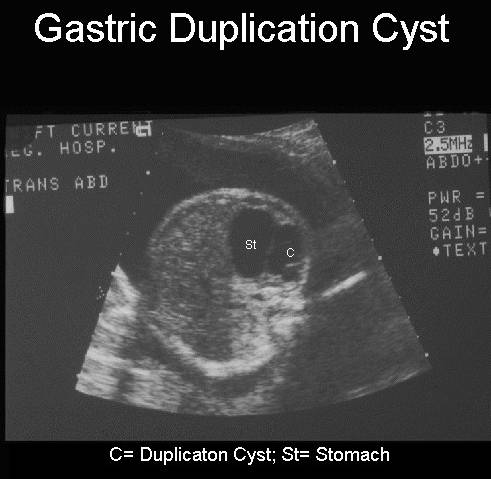
GASTRIC DUPLICATION
CYSTS
|
Most gastric duplications are cystic and non-communicating found on the
greater curvature of the stomach close to the pylorus (1).
- Cystic abdominal mass.
- The wall of the cyst may have
an inner hyperechoic layer (mucosa),
and a hypoechoic outer layer (muscular layer)
(2).
- Usually posterior to the
stomach (3), anterior to the spleen and inferior to the left lobe of the
liver.
- No relationship to the
gallbladder or hepatobiliary system.
- Cyst was constantly seen from
24 weeks gestation even after fetal physiologic gastric emptying (see
above case seen in our department).
- Size of the cyst is extremely
variable (most are 3-6cm).
- Shape:
- 82% are cystic and noncommunicating.
- 18% are tubular and
communicated with the gastric lumen (4).
- Position:
- Majority occurs along
the greater curvature of the stomach, with the majority in the antrum.
- May be associated with an intraabdominal pulmonary sequestration and cystic adenomatoid malformation (5).
- Duplication of the esophagus
(4).
- Vertebral malformations (6).
- Aberrant pancreas (6).
- Neuroblastoma.
- Teratoma
of the stomach.
- Pancreatic pseudocyst.
- Boureau
M. Intestinal duplication. In: Navarro J, Schmitz J (eds). Pediatric gastroenterology. New York, Oxford
University Press
1992:404-410.
- Bidwell
JK, Nelson A. Prenatal ultrasonographic
diagnosis of congenital duplication of the stomach J Ultrasound Med 1986;5:589.
- Ozmen MN,
Onderoglu L, Ciftci AO
et.al. Prenatal diagnosis of gastric duplication
cyst. J Ultrasound Med 1997;16:219-222.
- Wieczorek
RL, Seiderman I, Ranson
JHC et.al. Congenital duplication of the stomach:
Review of English literature. Am J Gastroenterol
1984;79:597.
- Brink DA, Balsara
ZN. Prenatal detection of intra-abdominal pulmonary sequestration with
postnatal MRI correlation. Pediatr Radiol 1991;21:227-229.
- Parker BC, Guthrie J, France NE
et.al. Gastric duplications in infancy. J Pediatr Surg 1972;7:294.