|
SMALL BOWEL
OBSTRUCTION |
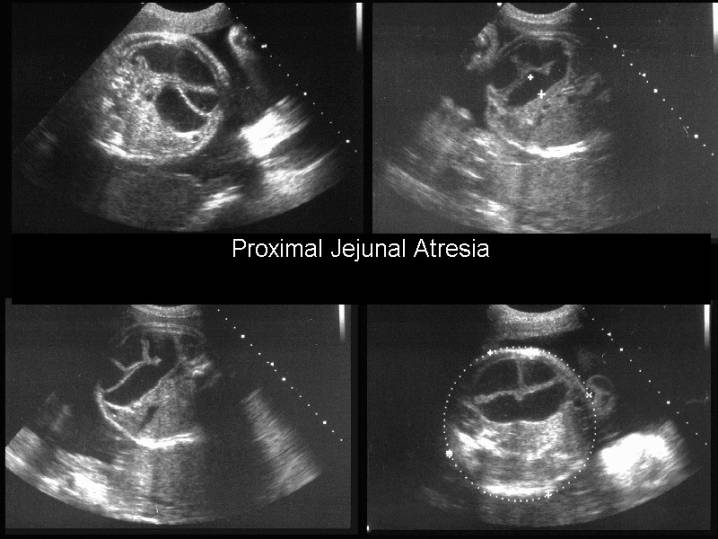
Jejunal and/or ileal atresia occurs in about 1 of 3,000 live births and is believed to be caused by an interruption of blood flow to the affected segment (11).
- Jejunal atresia - the atresias tend to be multiple and the jejunum has the capacity to dilate considerably before perforation occurs.
- Ileal atresias tend to be solitary and perforation occurs more readily with very little dilatation, (11-13). Fetal ascites seen in the setting of suspected bowel obstruction is likely to be caused by bowel perforation.
- The position of a dilated bowel loop is a poor predictor of whether or not it is small or large bowel.
- Focally dilated, isolated loops of bowel are sometimes seen in utero in the setting of small bowel atresia and may mimic cysts (14).
- Ileal atresia may be occult on early antenatal sonography and to come to attention only after delivery (15).
ETIOLOGY
|
- Mechanical obstruction:
- Intestinal atresia (usually due to an in utero vascular accident, secondary to hypotension, vascular accidents, intussusception, or vascular malformation).
- Intestinal stenosis.
- Intestinal Volvulus.
- Meconium ileus.
- Non - obstructive causes:
- Megacystis-microcolon-intestinal hypoperistalsis syndrome.
- Congenital chloridorrhea (1,2)
ULTRASOUND
|
- Most intestinal obstructive disorders do not occur until the third trimester (a second trimester scan is usually normal) (3).
- Multiple interconnecting overdistended bowel loops.
- Individual loops of bowel >15 mm in length or 7 mm in diameter (3,4).
- There is considerable variability in the appearance of the bowel in third trimester, such that a fetus with a prenatal diagnosis of intestinal obstruction, based solely on the presence of bowel dilatation may prove to be normal at birth (5).
- The number of dilated bowel loops depends on the level of obstruction (the lower the level the greater the number).
- Polyhydramnios (more common in higher obstructions).
- Peristalsis in the obstructed loops confirms that we are indeed looking at bowel.
- High small bowel obstructions may not be apparent until the late second or third trimester.
- In midgut
volvulus a whirlpool or snail sign is seen in utero (6-8).
The whirlpool sign is produced by the loop of bowel and its accompanying mesentery and mesenteric vessels that wrap around the superior mesenteric artery. Color or power doppler may help, by demonstrating the twisted mesenteric vessels that accompany the bowel and mesentery. Midgut volvulus and intestinal atresia often co-exist. Volvulus occurs when a loop of bowel rotates on an axis, causing an obstruction to the lumen and the mesenteric vessels. In utero, volvulus may occur when the mesentery is incompletely affixed to the retroperitoneum (9). The resultant ischemia leads to atresia of the associated bowel. - Complications include bowel obstruction, perforation and ischemic necrosis due to vascular compromise.
|
|
|
|
|
|
|
|
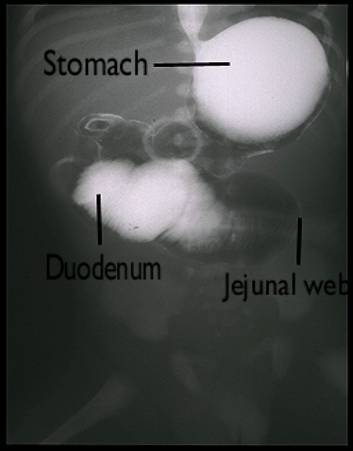
Postnatal
Barium study of Proximal Jejunal Atresia/ |
|
|
Jejunal web |
|
|
Proximal ileal obstruction – atresia
at surgery. Etiology
probably vascular |



Rotational Abnormalities |
||
Non Rotation |
Malrotation |
Reversed Rotation |
|
· Midgut returns to abdominal cavity after rotating only 1800 and not 2700. · Post-arterial (colonic) limb reenters the abdominal cavity first instead of last. |
· Rotation occurs but is incomplete. · Prearterial segment returns to the abdomen first and is usually in a normal position. |
· Postarterial segment of the midgut returns to the abdomen first. · This unwinds the normal counterclockwise rotation that occurred during the first stage and substitutes a final clockwise rotation of 900. |
|
· Small bowel on right side of abdomen. ·
|
· Degree of malrotation is indicated by position of cecum: · Cecum may be on left side, higher than normal on the right side or in an intermediate position. |
· Transverse colon lies behind the duodenum and is separated from it by the SMA. |
Malrotation with midgut volvulus
If mesenteric fixation of bowel does not occur in a normal fashion, nonrotation or malrotation of bowel has occurred.
Without normal fixation of bowel into position, there is increased risk of displacement and subsequent bowel ischemia because of twisting of mesenteric vessels. This can occur at any time beginning in fetal life and continuing on into adulthood.
- If midgut volvulus occurs in the fetus, it may be sonographically visible as dilated loops of bowel (16-18).
- Unfortunately, it is difficult, if not impossible, to distinguish midgut volvulus, a surgical emergency, from other nonurgent causes of bowel obstruction.
- Malrotation has been described in fetuses shown to have large intraabdominal masses, suggesting that the presence of the mass did not allow normal bowel fixation to occur (19).
DIFFERENTIAL
DIAGNOSIS
|
- Multicystic renal dysplasia.
- Dilated tortuous ureter.
- Normal caliber large bowel (large bowel has a more peripheral location).
REFERENCES
|
- Langer JC,
- Lundkvist K, Ewald U, Lindgren PG. Congenital chloride diarrhoea: a prenatal differential diagnosis of small bowel atresia. Acta Pediatr 1996;85:295-298.
- Ogunyemi D. Prenatal ultrasonographic diagnosis of ileal atresia and volvulus in a twin pregnancy. J Ultrasound Med 2000;19:723-726.
- Nyberg DA, Mack LA, Patten RM et.al. Fetal bowel - normal sonographic findings. J Ultrasound Med 1987;6:3-6.
- Lau TK, Fung HYM, Fung TK. Fetal bowel dilatation: Report of three cases with different outcomes. Aust NZ J Obstet Gynaecol 1997;37:323.
- Pracros JP, Sann L, Genin G et.al. Ultrasound diagnosis of midgut volvulus: the whirlpool sign. Pediatr Radiol 1992;22:18-20.
- Shimanuki Y, Aihara T, Takano H et.al. Clockwise whirlpool sign at color doppler US: an objective and definitive sign of midgut volvulus. Radiology 1996;199:261-264.
- Yoo
S -J, Park W, Cho SY et.al.
Definitive diagnosis of intestinal volvulus in utero. Ultrasound Obstet Gynecol 1999;13:200-203.
- Nyberg
DA, Mahony BS, Pretorius
DH. Diagnostic ultrasound of fetal anomalies: text and atlas.
- K.L. Moore and T.V.N. Persaud, The digestive system. In: K.L. Moore and
T.V.N. Persaud, Editors, The Developing Human:
Clinically Oriented Embryology ((ed 7).),
Saunders,
- R.J. Touloukian, Diagnosis and treatment of jejunoileal atresia. World J Surg 17 (1993), pp. 310–317.
- S. Lyrenas, S. Cnattingius and B. Lindberg, Fetal jejunal atresia and intrauterine volvulus—A case report. J Perinat Med 10 (1982), pp. 247–248.
- O. Bahgat, M. Lev-Gur and M.Y. Divon, Prenatal ultrasound diagnosis of intestinal obstruction: A case report. Am J Perinatol 6 (1989), pp. 324–325.
- A. Kubota, T. Nakayama, T. Yonekura et al., Congenital ileal atresia presenting as a single cyst-like lesion on prenatal sonography. J Clin Ultrasound 28 (2000), pp. 206–208.
- R.B. Parad, K. Applegate, P.M. Doubilet et al., Occult fetal bowel obstruction: Ileal atresia presenting in a newborn infant after normal antenatal sonography. J Ultrasound Med 14 (1995), pp. 161–163.
- N. Samuel, D. Dicker, D. Feldberg et al., Ultrasound diagnosis and management of fetal intestinal obstruction and volvulus in utero. J Perinat Med 12 (1984), pp. 333–337.
- B. Weinberg and E.E. Diakoumakis, Three complex cases of foregut atresia: Prenatal sonographic diagnosis with radiographic correlation. J Clin Ultrasound 13 (1985), pp. 481–484.
- S.J. Yoo, K.W. Park, S.Y. Cho et al., Definitive diagnosis of intestinal volvulus in utero. Ultrasound Obstet Gynecol 13 (1999), pp. 200–203.
- R. Littlewood Teele, P.W. Pease and R.S. Rowley, Malrotation in newborns following antenatal diagnosis of intra-abdominal cyst. Pediatr Radiol 28 (1998), pp. 717–721.