|
LARGE BOWEL
OBSTRUCTION |
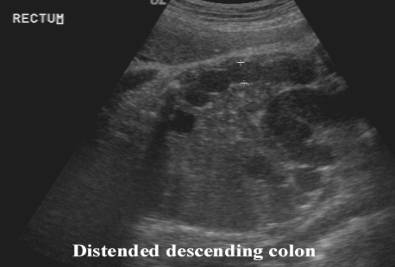
Large bowel obstruction is more difficult to diagnose than small bowel
obstruction because of the wide range in the normal diameter of the fetal
colon.
ETIOLOGY |
- Anorectal atresia.
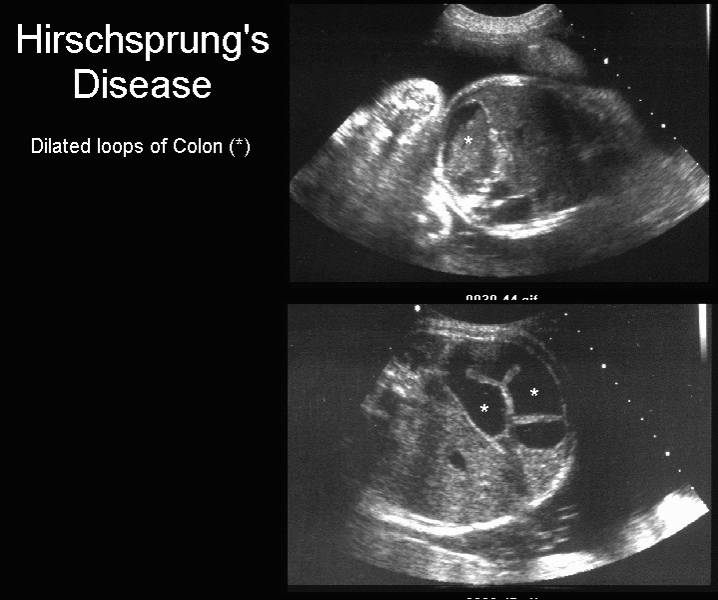
- Hirschsprung's disease.
- Meconium plug syndrome.
ULTRASOUND |
- Diagnosis must be made with caution in view of the wide variation in size and prominence of the normal colon.
- May reach 18 mm or more at term (1).
- V- or U-shaped segments of bowel, and intraluminal colonic calcifications have been described associated with anorectal atresia (2-4).
|
|
|
|
|
|
|
|
V- or U-
shaped segments of bowel |


PITFALL IN THE DIAGNOSIS OF LARGE BOWEL OBSTRUCTION |
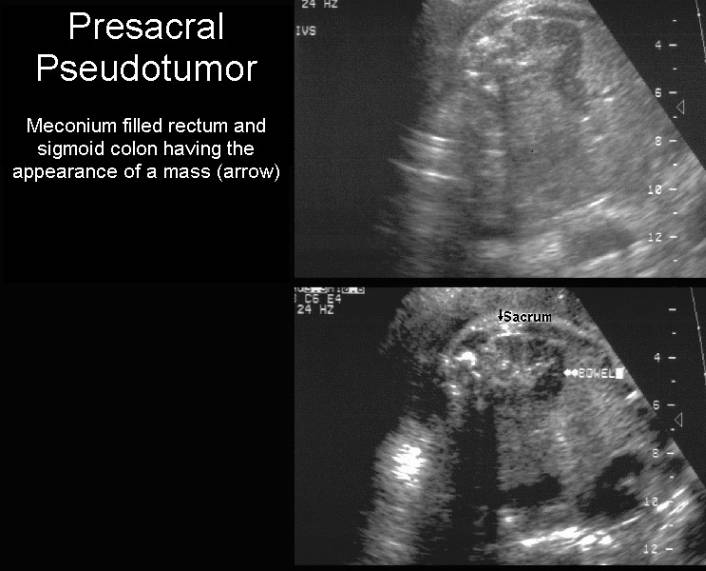
The Presacral Pseudomass.
Axial scans through the rectum can give the spurious impression that a presacral mass i.e. sacrococcygeal teratoma or anterior meningocele is present. The transducer needs to be rotated into an oblique position which will demonstrate the typical appearance of the rectosigmoid colon.
Do not mistake normal colon for a pseudomass.
6.3% of normal third trimester fetuses may have a hypoechoic presacral mass
measuring 15-30mm. This represents the meconium filled rectum in the term fetus.
|
|
REFERENCES |
- Nyberg DA, Mack LA, Patten RM et.al. Fetal bowel - normal sonographic findings. J Ultrasound Med 1987;6:3-6.
- Shalev E, Weiner E, Zuckerman H. Prenatal ultrasound diagnosis of intestinal calcifications with imperforate anus. Acta Obstet Gynecol Scand 1983;62:95-96.
- Grant T, Newman M, Gould R et.al. Intraliminal colonic calcifications associated with anorectal atresia. J Ultrasound Med 1990;9:411-413.
- Harris RD, Nyberg DA, Mack LA et.al. Anorectal atresia: prenatal sonographic diagnosis. AJR 1987;149:395-400.