|
HORSESHOE KIDNEY |
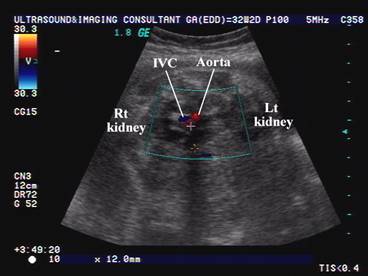
The horseshoe kidney results from fusion of the upper or lower poles of two distinct functioning kidneys to produce a horseshoe shaped organ that is contiguous across the midline anterior to the aorta and inferior vena cava (1-3).
- It is the most common renal fusion abnormality occuring in 1 in 500 persons.
- As with other fusion anomalies, it is more common in males (3).
- In this anomaly, the poles of the 2 kidneys are fused, usually the lower poles. The horseshoe kidneys’ polar fusion results in an isthmus of tissue (parenchymal or fibrous between the 2.
- 90% are fused at the lower pole and 10% are fused at the upper pole.
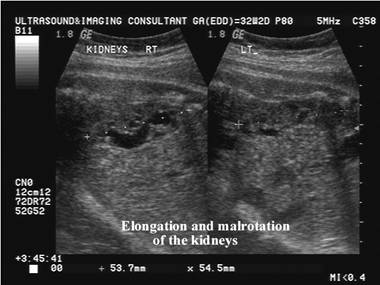
- The isthmus prevents normal renal rotation.
- It has its own blood supply.
- The usual position of the isthmus is at the junction of the aorta with the inferior mesenteric artery.
- The ureters usually exit the anteriorly postioned renal pelves to descend inferiorly
- The kidney is usually lower in position than a normal kidney and anterior to the aorta and inferior vena cava. In at least one third of cases, the horseshoe kidney is not discovered until autopsy.
- Most (90%) cases are asymptomatic. Wilson and Azmy (4) however, reported 15 of 20 children with horseshoe kidney presenting with symptoms and 9 requiring surgery. In another review of 30 caseS (5) twice as many patients were male; 22 cases presented with abdominolumbar pain, 12 with hematuria and 2 with pyuria. In 20 of those cases, the horseshoe kidney had associated renal stones and in one an upper urinary tract tumor.
EMBRYOLOGY |
This developmental anomaly occurs between 7 and 9 weeks of gestation (1). The intermediate mesoderm that gives rise to the metanephric blastema fails to separate. AS the ureteric bud grows cranially, they come into contact with the fused nephrogenic cords and nephrogenesis proceeds. With growth of the embryo, the ascent of the kidney is arrested as the isthmus of the kidney makes contact with the inferior mesenteric artery. Normal posterior rotation of the kidney is prevented by the fusion resulting in the renal pelves becoming orientated anteriorly. Fusion usually occurs at the lower poles. Upper and midpole fusion is rare.
Two theories of embryogenesis have been proposed.
· The classic theory involves mechanical fusion of two kidneys during organogenesis. The inferior poles of kidneys touch and fuse in the lower midline during the migration through the narrow fork of umbilical arteries (6).
· An alternative theory proposes that there is abnormal migration of posterior nephrogenic cells, which then coalesce to form the parenchymal isthmus (7,8). Teratogenic events involving the abnormal migration of posterior nephrogenic cells may be responsible for the increased incidence of related congenital anomalies and neoplasms associated with the isthmus of the horseshoe kidney (8).
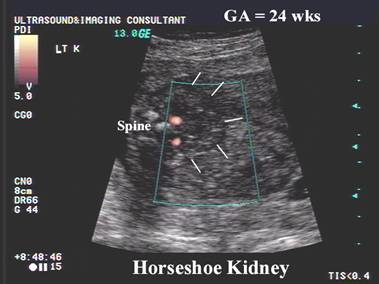
ULTRASOUND |
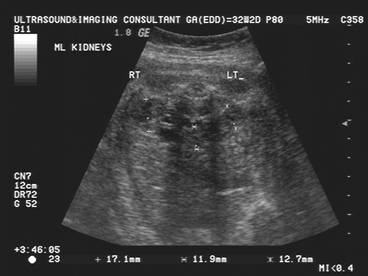
- Rarely diagnosed in utero (2) as the normal transverse image of the fetal kidneys are usually obtained at the level of the renal hilum. Inferior or superior fusion cannot therefore be appreciated.
- Continuous renal parenchyma across the midline - The fused isthmus is the most conclusive finding, but surrounding bowel echoes can obscure the isthmus in many fetal cases.
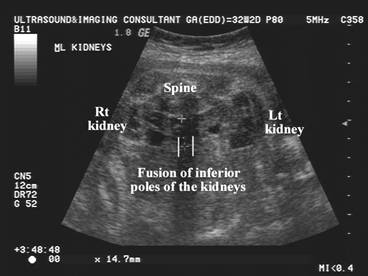
- Lower poles fuse anterior to the aorta.
- Malrotation of the kidneys with the renal pelves and ureters located more ventrally. This results in an abnormal longitudinal axis (19).
- The mean pelvic angle in horseshoe kidneys are 116 and 110 degrees (normal kidneys are 172 and 161 degrees) (19). 140 degrees is suggested as a discriminating criterion.
- The pelvis of horseshoe kidney has a more anterior location and is often more dilated than normal (corresponding to failure of medial renal rotation caused by fusion).
- Abnormal orientation of the adrenal glands.
|
|
|
|
|
|
|
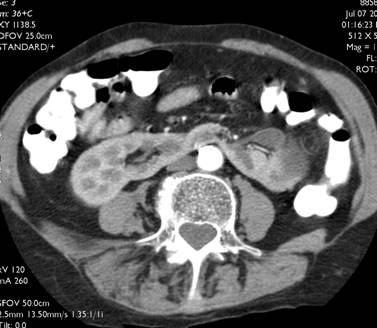
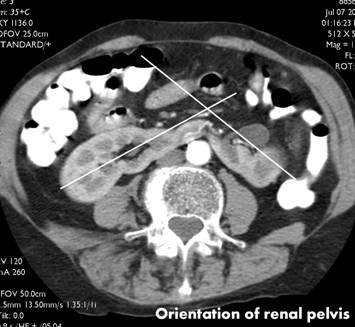
Horshshoe
kidney – CT scan |
|
|
|
|
|
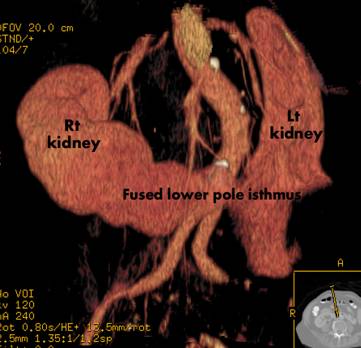
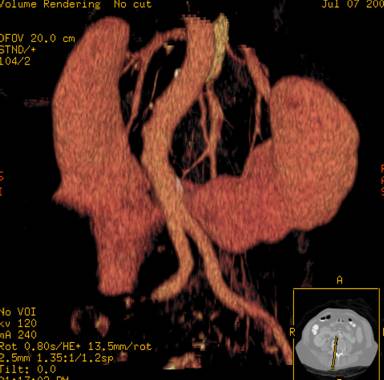
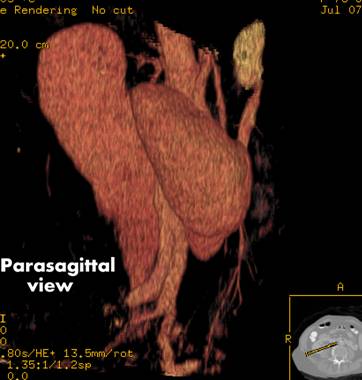
3D reconstructed images of horshshoe
kidney |
|
|
|
|
|
|
|



ASSOCIATIONS |
- Increased frequency in Turner's Syndrome (occurring in as many as 7%), trisomy 18 and trisomy 9 (9-11).
- Horseshoe kidneys occur more commonly in patients with Trisomy 18, and neural tube defects.
- One third of patients with horseshoe kidneys have other abnormalities including those of the GU, GI, respiratory, and skeletal systems.
- Malignancy
- Wilms' tumor (the relative risks of each tumor are increased four fold).
- transitional cell carcinoma (the relative risks of each tumor are increased two fold).
- carcinoid tumor (the relative risks of each tumor are increased 62 fold) (12-14).
- Horseshoe kidney can be accompanied by other genitourinary anomalies, such as:
1. vesicoureteral reflux (50%),
2. duplication of ureters (10%),
3. hypospadia
4. undescended testis (4%),
5. bicornuate or septate uterus (7%) (9,15,16).
6. Horseshoe kidney is also frequently found in association with other congenital anomalies. Most commonly affected organs are cardiovascular, skeletal, and central nervous systems (9,16).
COMPLICATIONS |
· Horseshoe kidneys are at greater risk than normal kidneys for obstruction, usually at the ureteropelvic junction as well as vesicoureteral reflux, infection, urolithiasis, and malignancy.
· Because the pelvises are both extrarenal, they appear more patulous than usual even if not obstructed.
· Carcinoma of the renal pelvis is more common among horseshoe kidney patients. Wilm’s tumor (which is 2–8 times more frequent in children with horseshoe kidneys) has a reported predilection for the horseshoe kidney’s isthmus.
· Hydronephrosis is caused by ureteropelvic junction obstruction, which may be due to the high insertion of the ureter into the renal pelvis, crossing of the ureter over the isthmus, and ureteric entrapment by aberrant vessels.
· renal stones.
· infection (17,18).
REFERENCES |
- Barakat Ay, Awazu M, Fleisher AC. Antenatal diagnosis of renal abnormalities: A review of the state of the art. South Med J 1989;82:229.
- Sherer DM, Cullen JBH, Thompson HO et.al. Prenatal sonographic findings associated with a fetal horseshoe kidney. J Ultrasound Med 1990;9:477-479.
- C. Wilson and A.F. Azmy, Horseshoe kidney in children. Br J Urol 58 (1986), pp. 361–363
- J. Walter and J. McGahan, Mesoblastic nephroma: prenatal sonographic detection. J Clin Ultrasound 13 (1985), pp. 686–689.
- Sadler TW. Urogenital System. In Langman’s Medical Embryology (7th edition), Williams and Wilkins, Baltimore 1995;272-311.
- Domenech-Mateu JM, Gonzalez-Compta X. Horseshoe kidney: a new theory on its embryogenesis based on the study of a 16-mm human embryo. Anat Rec 1988; 222: 408-417.
- Hohenfellner M, Schultz-Lampel D, Lampel A, Steinbach F, Cramer BM, Thuroff JW. Tumor in the horseshoe kidney: clinical implications and review of embryogenesis. J Urol 1992; 147: 1098-1102.
- Bauer SB. Anomalies of the
upper urinary tract. In
- Lippe B, Geffner ME, Dietrich RB, Boechat MI, Kangarloo H. Renal malformations in patients with Turner syndrome: imaging in 141 patients. Pediatrics 1988; 82: 852-856.
- Sandoval R, Sepulveda W, Gutierrez J, Be C, Altieri E. Prenatal diagnosis of nonmosaic trisomy 9 in a fetus with severe renal disease. Gynecol Obstet Invest 1999; 48: 69-72.
- Buntley D: Malignancy associated with horseshoe kidney. Urology 1976; 8: 146-148.
- Mesrobian HG, Kelalis PP, Hrabovsky E, Othersen HB Jr, deLorimier A, Nesmith B. Wilms' tumor in horseshoe kidneys: a report from the National Wilms' tumor Study. J Urol 1985; 133: 1002-1003.
- Krishnan B, Truong LD, Saleh G, Sirbasku DM, Slawin KM. Horseshoe kidney is associated with an increased relative risk of primary renal carcinoid tumor. J Urol 1997; 157: 2059-2066.
- Boatman DL, Kolln CP, Flocks RH. Congenital anomalies associated with horseshoe kidney. J Urol 1972; 107: 205-207.
- Zondek LH, Zondek T. Horseshoe kidney and associated congenital malformations. Urol Int 1964; 18: 347-356.
- Glenn JF. Analysis of 51 patients with horseshoe kidney. N Engl J Med 1959; 261: 684-687.
- Pitts WR, Muecke EC. Horseshoe kidney: a 40 year experience. J Urol 1975; 113: 743-746.
- Cho JY, Lee y –H, Toi A. et.al. Prenatal diagnosis of horseshoe kidney by measurement of renal pelvis angle. Ultrasound Obstet Gynecol 2005;25:544-558.