|
RENAL TUMORS -
MESOBLASTIC
NEPHROMA -
WILMS
TUMOR |
|
1. MESOBLASTIC NEPHROMA - (renal hamartoma
or leiomyomatous hamartoma)
(1-5) |
- Usually presents in the first year of life as an abdominal mass.
- Although it is a benign tumor and nephrectomy thought to be curative, atypical types have been rarely reported to recur or metastasize after nephrectomy.
ULTRASOUND
|
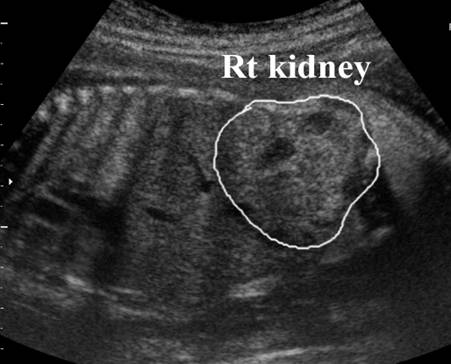
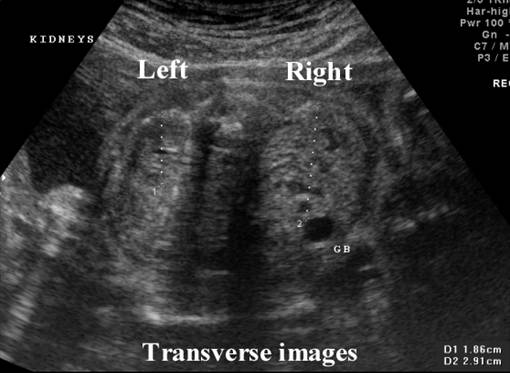
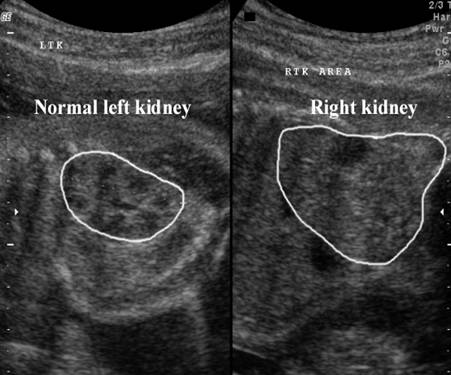
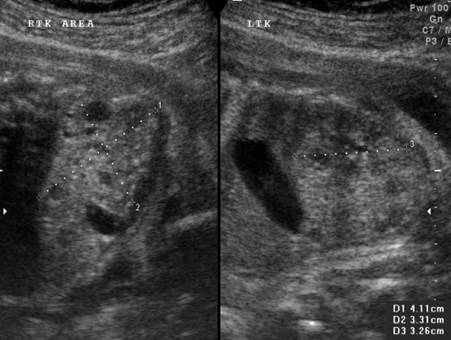
- Large and solitary tumor that is almost always unilateral.
- Predominantly solid that may completely replace the kidney. It may be difficult to detect antenatally as it is contiguous with normal nephrons and does not have a well-defined capsule.
- Hyperechoic or hypoechoic.
- Occasionally small cystic spaces may be present (this corresponds to areas of hemorrhage or cystic degeneration).
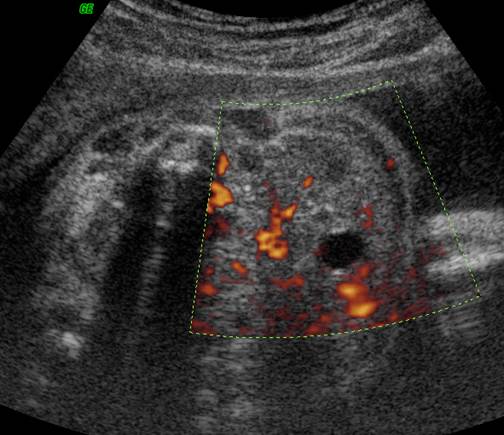
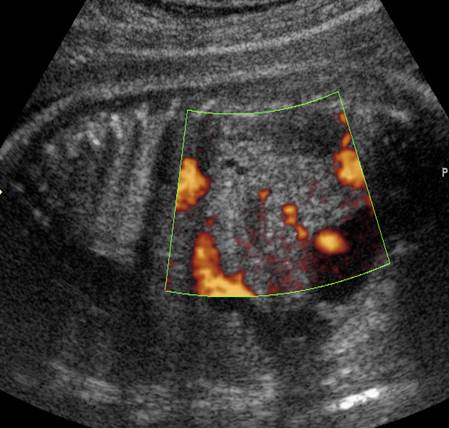
- Polyhydramnios is frequently present, and is thought to be due to the vascular nature of the lesion that results in increased renal perfusion and increased fetal urine production (6,9).
- Mesoblastic nephroma has been reported to be complicated by hydrops fetalis (14-16) and although the exact etiology remains uncertain, it may be that congenital mesoblastic nephroma is angiomatous and consequently the hydrops is due to high output cardiac failure (16).
- The sonographic findings of mesoblastic nephroma and of Wilms
 tumor
are similar (17) and the distinction can be made only
pathologically. However, the age of presentation provides an important
differentiating factor, as Wilms tumor is
exceptionally rare in the neonate.
tumor
are similar (17) and the distinction can be made only
pathologically. However, the age of presentation provides an important
differentiating factor, as Wilms tumor is
exceptionally rare in the neonate. - Magnetic resonance imaging has advantages over sonography because it is able to provide better tissue contrast and a variety of imaging planes regardless of the fetal orientation (18). It may be particularly useful in situations in which sonographic findings are impaired (18) (e.g. maternal obesity or abdominal scars, which impair ultrasound scanning, oligohydramnios, fetal head engagement).
|
|
Case
1 |
|
Case 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|




|
2.
WILM’S TUMOR (5, 7-8) |
Wilms tumor (nephroblastoma) is an embryonal neoplasm consisting of blastemal, stromal and epithelial elements. Although they are very rare in the neonatal period, over 75% of affected children are under 4 years of age (10). The mean age of presentation is 3.5 years of age (11). Congenital Wilms tumors are rare with an incidence of 0.16% of all cases of Wilms tumor (12).
Cytogenetic studies (13) has demonstrated a role for chromosome 11 in the pathogenesis of Wilms tumor. Closely linked WT1 and Wit1 genes are located at 11p13. WT1 gene appears to be involved in normal genitourinary organogenesis. Abnormalities in expression occur in 10% of cases of nephroblastoma. WAGR syndrome is characterized by a constitutional deletion. WT2 gene is located at 11p15 and abnormalities of expression are responsible for Beckwith-Wiedermann syndrome.
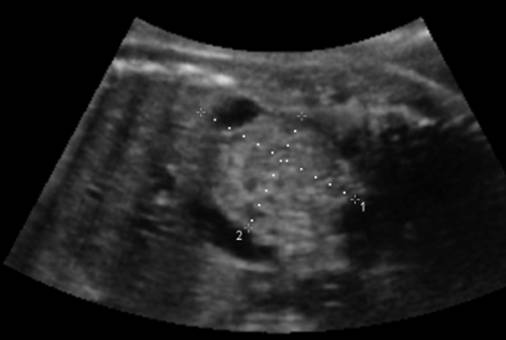
- Solid, echogenic well encapsulated tumor.
- Well defined margins (unlike the mesoblastic nephroma).
- Anechoic areas due to hemorrhage and necrosis may be present.
- Usually unilateral, rarely bilateral (5-10% of cases).
- Polyhydramnios (8).
- Hydrops is rare (12).
|
|

ASSOCIATED ANOMALIES (15% OF CASES)
|
- Hemi-hypertrophy (total, segmental or crossed) of the body is more common with bilateral tumors but is not present at birth and therefore cannot be diagnosed antenatally.
- Trisomy
18 and Turners syndrome have been reported in conjunction with Wilm's tumor (8).
- Beckwith-Wiedermann syndrome.
- Perlman syndrome.
- Denys-Drash syndrome (AD, pseudohermaphroditism,
diffuse mesangial sclerosis and gonadal dysgenesis).
- WAGR (sporadic, Wilms tumor, aniridia, genitourinary anomalies, mental retardation).
DIFFERENTIAL DIAGNOSIS
|
- Congenital mesoblastic nephroma.
- Adrenal
neuroblastoma.
- Adrenal
hemorrhage.
- Retroperitoneal teratoma.
REFERENCES
|
- Guilian BB. Prenatal ultrasonographic diagnosis of fetal renal tumors. Radiology 1984;152:69.
- Walter JP, McGahan JP. Mesoblastic nephroma: prenatal sonographic detection. J Clin Ultrasound 1985;13:686.
- Apuzzio JJ, Unwin W, Adhate A et.al. Prenatal diagnosis of fetal renal mesoblastic nephroma. J Ultrasound Med 1983;2:555.
- Blank E, Neerhout RC, Burry KA. Congenital mesoblastic nephroma of polyhydramnios. JAMA 1978;240:1504.
- Ohmichi M, Taska K, Sugita N et.al. Hydramnios associated with congenital mesoblastic nephroma: Case report. Obstet Gynecol 1989;74:469-471.
- Jaffe MH, White SJ, Silver TM et.al. Wilm's tumor: Ultrasonic features, pathologic correlation, and diagnostic pitfalls. Radiology 1981;140:147.
- Suresh I, Suresh S, Arumugam R et.al. Antenatal diagnosis of Wilm's tumor. J Ultrasound Med 1997;16:69-72.
- Holley G, Labuski
M, Kasales C. Congenital mesoblastic
nephroma. Antenatal and postnatal sonographic appearance with pathologic correlation.
JDMS 1997;13:291-293.
- Beckwith
JB. Wilms tumor and other renal tumors of
childhood: a selective review from the national Wilms
tumor study Pathology center. Human Pathol 1983;14:481-492.
- Vadeyar S, Ramsay M, James D et.al.
Prenatal diagnosis of congenital Wilms tumor
presenting as fetal hydrops. Ultrasound Onstet Gynecol 2000;16:80-83.
- Thorner PS, Squire JA. Molecular genetics in the diagnosis and prognosis of solid pediatric tumors. Pediatr Dev Pathol 1998;1:337-365.
- Yuan-Chi L, Yuen-Lun M, Chung-Chen C et.al. The presence of hydrops fetalis in a fetus with congenital mesoblastic nephroma. Prenat Diagn 1996; 16: 363-5
- Angulo JC, Lopez JI, Ereno C et.al. Hydrops fetalis and congenital mesoblastic nephroma. Child Nephrol Urol 1991; 11: 115-6
- Gray ES. Mesoblastic nephroma and nonimmunological hydrops fetalis. Pediatr Pathol 1989; 9: 607-9
- Applegate KE, Ghei M, Perez-Atayde AR. Prenatal detection of a Wilms tumor. Pediatr Radiol
1999; 29: 65-7
- Kubik-Huch RA, Huisman TA, Wisser J et.al. MR imaging of the fetus. AJR Am J Roentgenol 2000; 174: 1599-606