|
ULTRASOUND OF
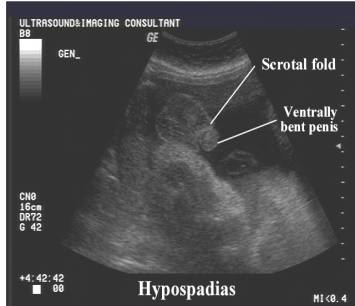
HYPOSPADIAS |
- Prenatal diagnosis is generally made in the third trimester, if good genital visualization has been obtained, although it is possible to suspect the diagnosis during the early second trimester (7,8). Most prenatally diagnosed cases have been attributed to distal hypospadias with ultrasound findings of anomalous distal morphology of the penis, small lateral folds, small penis with ventral incurvation or an anomalous urinary stream (9).
- Despite its frequency, hypospadias is often not identified antenatally and has only been described in a few papers (2-7).
- The normal penile shaft has a smooth tapering appearance.
- In hypospadias the tip of the penis is blunted and bulbous (corresponding to the dorsal hood that is over the glans due to the deficient prepuce that is present ventrally).
- Small penile shaft with two echogenic lines corresponding to small lateral folds belonging to the dermal remains of the prepuce (dorsal hood)
- Slight ventral or lateral curvature of the penile shaft (slight curvature may occur in the normal penis).
- Two parallel echogenic lines corresponding to lateral
folds of the dermal remains of the prepuce (dorsal hood). Depending on the
location of the meatus and the degree of penile curvature, these oblique
raphes end at the apex of a small skin cone or peaks of a cowl-shaped monk
 s
hood (have described as cobra eyes).
s
hood (have described as cobra eyes). - There may / may not be a tethering fibrous band, the chordee.
- The glans may extend beyond the prepuce (due to an incomplete or dorsal prepuce commonly found with most types of hypospadias).
- Urethral canal may be traced to an opening proximal to the glans (6).
- Fetal micturition occurring proximal to the glans may be demonstrated on gray scale (6) or color doppler images. The stream is fan-shaped and not linear.
- “Tulip sign” - represents the severe curvature of the penis in association with penoscrotal transposition of a bifid scrotum. Thus, this sign indicates the most severe form of hypospadias.
|
|
|
|
|
|


- Testis and scrotum usually normal.
REFERENCES |
- Kallen B, Bertollini R, Castilla et.al. A joint international study on the epidemiology of hypospadias. Acta Paediatr Scand Suppl 1986;324:152.
- Benacerraf BR, Saltzman DH, Mandell J. Sonographic diagnosis of abnormal genitalia. J Ultrasound Med 1989;8:613-617.
- Hogdall C, Siegel Bartelt J, Toi A et.al. Prenatal diagnosis of Opitz (BBB) syndrome in the second trimester by ultrasound detection of hypospadias and hypertelorism. Prenat Diagn 1989;9:783-793.
- Thomas D, Brat M, Camacho E. Hypospadias. Fetus 1993;3(1), 7562:1-4.
- Smulian JC, Rodis JF, Campbell WA et.al Hypospadias. Fetus 1993;3(4), 7562:5-10.
- Smulian JC, Scorza WE, Guzman ER et.al. Prenatal sonographic diagnosis of mid shaft hypospadias. Prenat Diagn 1996;16:276-280.
- Sides D, Goldstein RB, Baskin L et.al. Prenatal diagnosis of hypospadias. J Ultrasound Med 1996;15:741-746.
- Bronshtein M, Riechler A, Zimmer EZ. Prenatal sonographic signs of possible fetal genital anomalies. Prenat Diagn 1995; 15: 215–9.
- Devesa R, Munoz A, Torrents
M, Comas C, Carrera JM. Prenatal diagnosis of isolated hypospadias. Prenat
Diagn 1998; 18: 779–88