|
ULTRASOUND OF FETAL
OVARIAN CYSTS |
- Female fetus.
- Cyst size variable (2-8cm).
- Above and distinct from urinary bladder.
- Below and distinct from fetal stomach and gallbladder.
- Exclude abnormalities of the spine, GI tract and urinary system.
- 85-90% are cystic (follicular or luteinic origins).
- 10-15% are organic (< 3% are carcinomas and 7-12% are teratomas, mucinous or serous cystadenomas).
Ovarian carcinoma has been rarely reported:
· Ziegler et.al. (1945) (1) – bilateral ovarian carcinoma in a 30 week fetus.
· Henrion et.al. (1987) (2) – ovarian malignancy represents 3.5% of neonatal ovarian masses.
|
|
|
|
|
|



CLASSIFICATION / ULTRASOUND |
Six classes are described according to sonographic and pathologic appearance of the cyst (1-9).
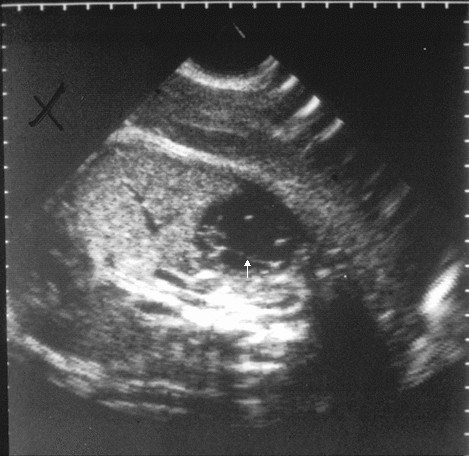
- Simple and anechoic with an imperceptible wall.
- May have a fluid - debris level.
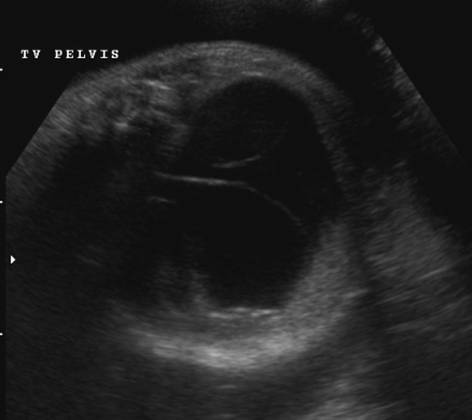
- Cyst with a retracting clot.
- Cyst with septations (considered simple if no internal echoes are present).
- Solid appearing.
- “Daughter cyst” – cyst within or outside the main cyst (3,9).
· Lee et.al. (3) Sensitivity 82%, specificity 100% confirming ovarian origin.
· Thought to be due to hormonal dysfunction leading to genesis of follicular and lutenic cysts. Corresponds to an excessively developing intra-ovarian follicle just before ovulation.
· Appearance identical to a Graffian follicle with cumulus oophorus.
Groups 2 to 5 are considered complicated.
|
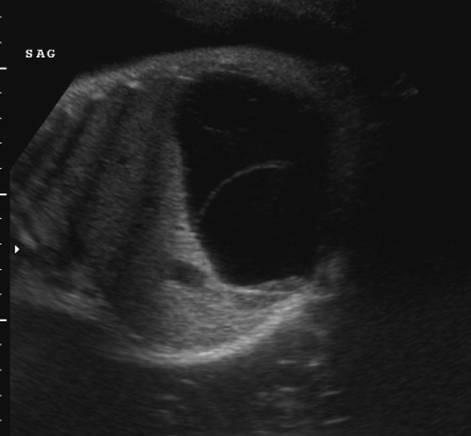
Simple ovarian cyst |
|
|
|
|
|
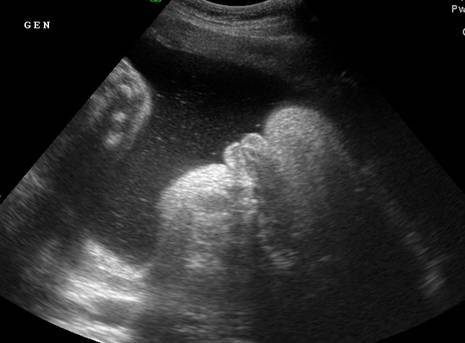
Ovarian torsion |
|
|
|
|
|
|
Ovarian cyst
with retracting clot |
|
|
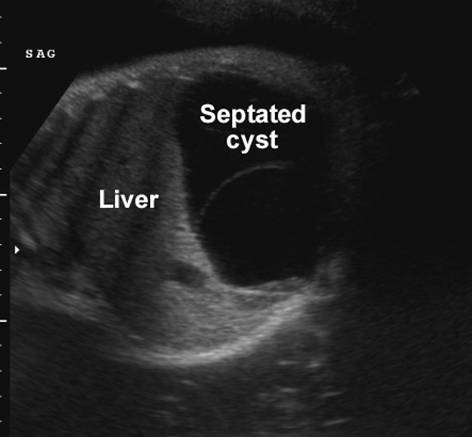
Complex
ovarian cyst with septation |
|
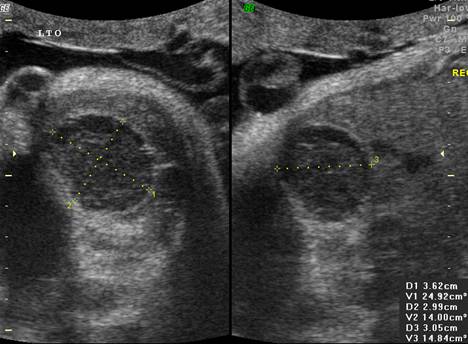
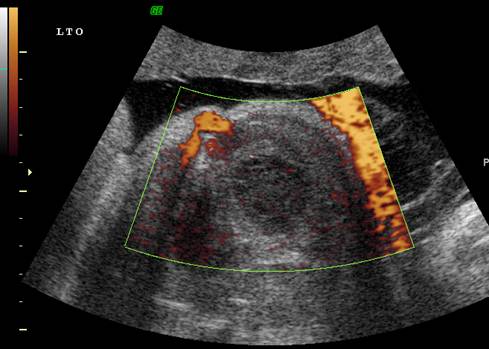
Ovarian torsion |
|
|
|
Cystic mass Hemorrhage within Separate from
kidney and stomach |
|
|
Retracting
clot within Avascular on power doppler |
|
|
|
|
|
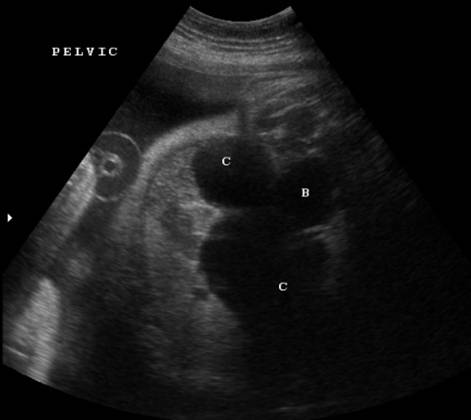
Female fetus |
|
Bilateral
multiseptated ovarian cysts C – cyst B - bladder |
|
|
|
|
|
|
|

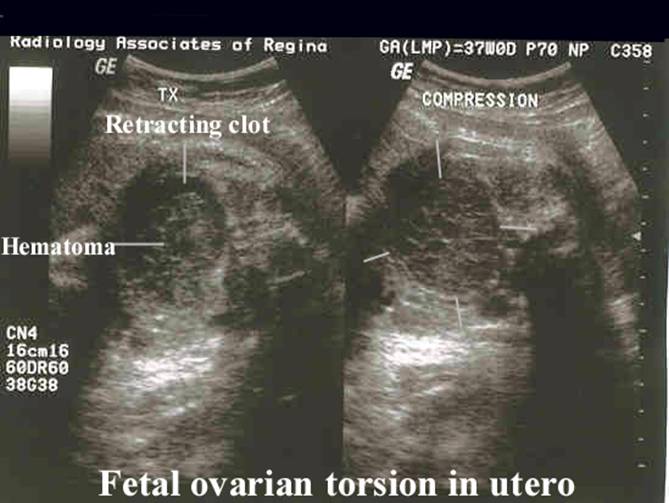



SONOGRAPHIC SIGNS OF TORSION (6-8) |
- Torsion ocured prenatally in 38% of cases in Brandt’s series (10).
- Septae developing within simple cyst (representing strands of necrotic cells that have separated from the wall of the cyst due to ischemia).
- Irregular echogenic material within the cyst due to intracystic hemorrhage.
- Fluid debris level develops as the hematoma liquefies.
- A retracting clot forms at the bottom of the cyst due to organization of the hematoma.
- Ascites if rupture occurs.
REFERENCES |
- Ziegler EE. Bilateral ovarian carcinoma in a thirty week fetus. Arch Pathol 1945:40:433-434.
- HenrionR,
Helardot PG. In utero disgnosis
of cysts of the ovary (in French). Ann Pediatr (
- Lee H-J, Woo S-K, Kin J-S et.al. Daughter cyst sign: a sonographic sign of ovarian cyst in neonate, infants and young children. Am J Roentgenol 2000;174:1013-1015.
- Garel L, Filiatrault D, Brandt M et.al. Antenatal diagnosis of ovarian cysts: natural history and therapeutic implications. Pediatr Radiol 1991;21:182-184.
- Shozu M, Akasofu K, Yamashiro G et.al. Changing ultrasonographic appearance of a fetal ovarian cyst twisted in utero. J Ultrasound Med 1993;12:415-417.
- Widdowson DJ, Pilling DW, Cook RC. Neonatal ovarian cysts: therapeutic dilemma. Arch Dis CHILD 1988;63:737.
- Gaudin J, Treguilly CL, Parent P et.al. Neonatal ovarian cysts. Twelve cysts with antenatal diagnosis. Pediatr Surg Int 1988;3:158.
- Quarello E, Gorinicourt G, Merrot T et.al. The “daughter cyst” sign: a sonographic clue to the diagnosis of fetal ovarian cyst. Ultrasound Obstet Gynecol 2003;22:431-436.
- Brandt ML, Luks FI, Filatrault D et.al. Surgical indications in antenatally diagnosed ovarian cysts. J Pediatr Surg 1991;26:276-282.