|
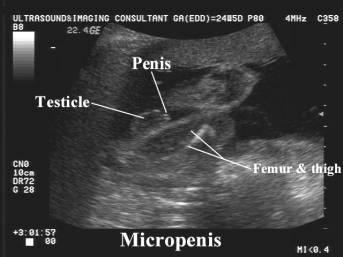
MICROPENIS |
Micropenis
is defined as a normally structured penis that is below the normal size range
for an infant (penile length < 2.5 standard deviations below mean for
age and race). Normally, the length of a newborn boy's penis is between 2.8 to 4.2
centimeters with a circumference of 0.9 to 1.3 centimeters. This measurement is
taken by carefully stretching the penis and measuring from the tip of the penis
to the base of the penis. A penile length of less than 1.9 centimeters is
usually considered micropenis.
This condition may be considered a minor
form of ambiguous genitalia with correlated medical and psychological problems
similar to those of the major intersex form. The scrotum usually is normal, but
testes often are small and undescended. In a few cases, the corpora cavernosa
are severely hypoplastic. Measurement of penile length is very important in
differentiation of the various types of pseudomicropenis (e.g.the buried penis in
the obese infant and the penis concealed by an abnormal skin attachment).
|
|
|
|
|
|

ETIOLOGY |
Micropenis can occur alone, but usually occurs in combination with other
disorders. Hormone disorders that cause an abnormal level of hormones, which are
involved in development of the sexual organs, may be seen in combination with
micropenis. This can involve the pituitary gland or the hypothalamus. Syndromes
where this is evident include the following:
- Idiopathic micropenis - endocrine analysis demonstrates a normal hypothalamic-pituitary-testicular axis.
- Hypogonadotropic hypogonadism (most common cause; 50% of cases). Secretion of gonadotropin-releasing hormone (GnRH) by the hypothalamus is impaired. This leads to decreased pituitary secretion of luteinizing hormone and follicle-stimulating hormone, depriving the testis of its stimulus to secrete testosterone. This pathogenesis exists in some hypothalamic dysfunctions, such as Kallmann syndrome or Prader-Willi syndrome.
- Kallmann syndrome - A complex genetic disorder that involves the hypothalamus (an important structure located in the brain that is responsible for the secretion of hormones and regulation of metabolism). Low GnRH and anosmia.
- Prader-Willi syndrome - A genetic disorder characterized by a decrease in sex hormones, obesity, short stature, small hands and feet and mental retardation.
- Lawrence-Moon-Biedl syndrome – obesity, mental retardation, pigmented retinopathy (blindness), polydactyly
- Rud syndrome – mental retardation, epilepsy, ichthyosis
- Androgen insensitivity syndrome (minimal) - an inherited defect in the gene on the X chromosome which causes recognition of the male hormone, testosterone. Receptors on the cells do not recognize the hormone, causing the penis to not grow. The scrotum may be bifid (appears to have two sections). During puberty, mild breast development may be present, and in adulthood, there may be a low sperm count. Most symptoms are treatable by intramuscular injections of testosterone. However, infertility may be present.
- Lawrence-Moon syndrome - An extremely rare genetic disorder that involves mental retardation, night blindness, and spastic paraplegia, which becomes worse over time.
- Micropenis secondary to hypergonadotropic hypogonadism (25% of cases) is associated with conditions in which the testes are impaired functionally and unable to respond to hypothalamic-pituitary stimulation.
- Testicular dysgenesis – HCG stimulation test and radiographic imaging may not detect; requires exploration to remove dysgenetic testes to prevent malignant degeneration; sporadic or familial.
- Klinefelter syndrome – testicular dysgenesis.
- Laurence-Moon-Biedl syndrome – can also be associated with hypergonadotropic hypogonadism.
- Multiple X syndromes
- Vanishing testis syndrome – intrauterine torsion; bilateral loss results in micropenis.
- Robinow syndrome - mesomelic dwarfism, dental anomalies.
- LH receptor defect/mutation
- Chromosomal anomalies:
- Klinefelter syndrome.
- Down syndrome.
- Translocations, deletions, trisomy involving chromosomes 8, 13, and 18.
- 69, XXY triploidy
- Isolated hormone
deficiencies (hypopituitarism):
- GnRH deficiency –may
occur without Kallmann syndrome.
- LH deficiency –
fertile eunuch syndrome; small penis, normal sized testes.
- Growth hormone
deficiency – both deficiency of hormone and effect (Laron dwarfism).
- Thyroid hormone
deficiency.
- ACTH deficiency –
leads to cortisol deficiency and circulatory collapse.
- Panhypopituitarism.
- Testosterone
underproduction (primary testicular failure).
- Androgen insensitivity - AR
mutation; usually associated with ambiguous genitalia.
- CNS abnormalities:
- Anencephaly.
- Congenital pituitary
aplasia.
- Agenesis of corpus
callosum.
- Septo-optic dysplasia.
- Occipital
encephalocele.
- Dandy-walker cystic
malformation of fourth ventricle.
- Cerebellar
malformations with ataxia.
- Other rare syndromes:
- Rud syndrome.
- Martsolf syndrome.
- Gorlin’s multiple
lentigenes syndrome.
- Robinow syndrome.
- Fanconi’s anemia.
- Smith-Lemli-Opitz
syndrome.
- Boucher-Neuhauser
syndrome.
- Mobius sequence.
REFERENCES |
- Aaronson IA: Micropenis: medical and surgical implications. J Urol
1994; 152(1): 4-14.
- Anhalt H, Neely EK,
Hintz RL: Ambiguous genitalia. Pediatr Rev 1996; 17(6): 213-20.
- Balaji KC, Caldamone AA, Rabinowitz R: Splenogonadal fusion. J Urol
1996; 156(2 Pt 2): 854-6.
- Bin-Abbas B, Conte FA, Grumbach MM: Congenital hypogonadotropic
hypogonadism and micropenis: effect of testosterone treatment on adult
penile size why sex reversal is not indicated. J Pediatr 1999; 134(5):
579-83.
- Hendren WH: The genetic male with absent penis and urethrorectal
communication: experience with 5 patients. J Urol 1997; 157(4): 1469-74.
- Moore PJ, Hawkins EP, Galliani CA: Splenogonadal fusion with limb
deficiency and micrognathia. South Med J 1997; 90(11): 1152-5.