|
ANATOMY OVERVIEW –
FIRST TRIMESTER |
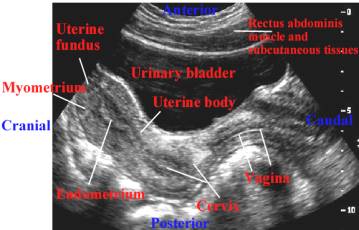
THE NORMAL UTERUS – Transabdominal
scan
|
|
|
|
|
|
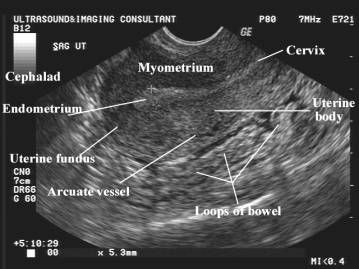
THE NORMAL
UTERUS – Transvaginal scan |
|
|
|
|
|
The uterus is a thick, pear-shaped muscular organ located between the two layers of the broad ligament laterally, the urinary bladder anterior and the rectosigmoid colon posteriorly.
The myometrium has a homogeneous echotexture with smooth borders. The transition between the endometrium and myometrium is delineated by an echo poor line, which is thought to represent the deeper more vascular layer of the inner myometrium. Normal arcuate vessels may be seen in the periphery of the uterus. These vessels bifurcate into radial branches, which supply blood throughout the uterus. The endometrium appears as a central line whose appearance and density are related to the phases of the menstrual cycle. After menstruation, when the majority of the decidual inner layer of the endometrium has been shed, only a fine cavitatory line present. As the endometrium thickens in the proliferative phase of the cycle, it becomes more prominent but remains echo poor. The endometrium continues to thicken and become more reflective as it enters the secretory phase presumable due to the glands filling with mucin and becoming tortuous. Towards the end of the cycle the endometrial shadow (which includes both the anterior and posterior endometrium) may reach 10 mm. |
|


|
4+4
weeks of gestation |
|
|
|
|
|
The first sonographic sign of an intrauterine pregnancy is a small sonolucent sac (chorionic cavity) surrounded by an echogenic rim of tissue (trophoblastic tissue and associated decidual reaction). Ultrasound is only able to detect an intrauterine gestational sac at approximately 4.5 to 5 weeks of gestation when the mean sac diameter reaches 2-3 mm. This early gestational sac contains chorionic fluid and within it develops the embryonic plate (and surrounding amnion) and the yolk sac. |
|
|
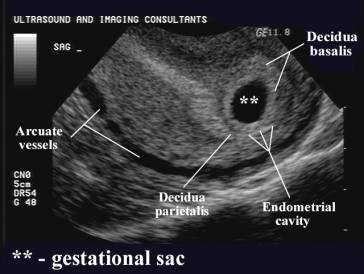
4+6
weeks of gestation |
|
|
|
|
|
This echogenic rim of tissue around the gestational sac consists of decidua basalis (villi on the myometrial or burrowing side of the conceptus) and the decidua capsularis or parietalis (villi covering the rest of the developing embryo). The interphases between the decidua capsularis and bright well vascularised endometrium is called the double decidual reaction and is represented by two concentric rings or crescents around the gestational sac. This implies that this is a true gestational sac associated with an intrauterine pregnancy. |
|
|
5+1
weeks of gestation |
|
|
|
|
|
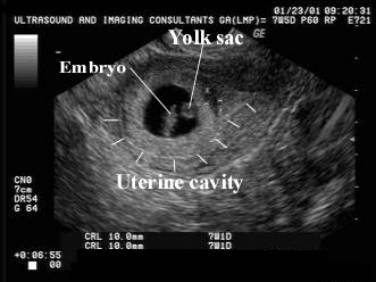
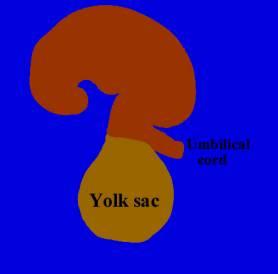
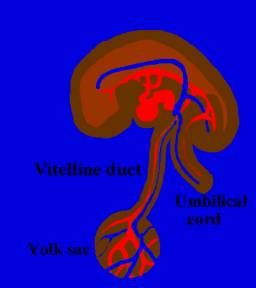
The yolk sac is the first visualized structure that is seen within the gestational sac. It lies within the chorionic cavity and is routinely seen from 5 weeks of gestation. It is attached to the embryo by the yolk stalk (vitelline duct). As the embryonic cavity begins to enlarge, the yolk sac (which is extra-amniotic) moves away from the embryo and eventually detaches from the yolk stalk, and is no longer constantly seen after 12 weeks of gestation. |
|
|
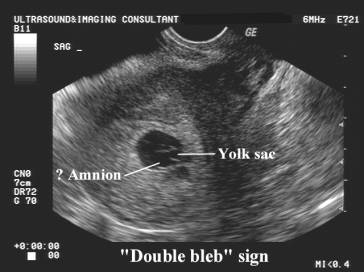
5+4
weeks of gestation |
|
|
|
|
|
|
|
|
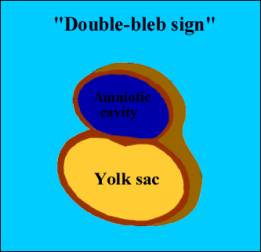
The “double-bleb sign” is a transient appearance that can be seen in the gestational sac. It is produced by the yolk sac and probably the amniotic cavity. The trilaminar embryo is not yet visible at this stage. |
|
|
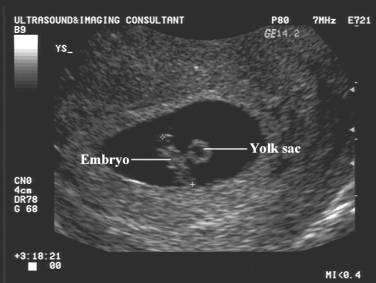
5+6
weeks of gestation |
|
|
|
|
|
|
|
|
The embryo can be detected when it is approximately 2 mm in length as an area of asymmetrical thickening of the yolk sac. It is not unusual to only demonstrate cardiac motion when the crown rump length (CRL) of the embryo reaches 5-6 mm. The amniotic sac is small and closely applied to the fetus and cannot be appreciated as a separate structure until there is sufficient amniotic fluid to separate the amnion from the embryo. |
|
|
6 weeks of
gestation |
|
|
|
|
|
By 6 weeks of gestation the crown rump length of the embryo reaches 5 mm and the embryo can be seen as a separate structure from the yolk sac and cardiac pulsations should be visible. The mean gestational sac size reaches 18-20 mm. |
|
|
7 weeks of
gestation |
|
|
|
|
|
Limb buds are embryologically recognizable during the seventh week of gestations projecting at ninety degrees off the body. The joints become apparent at 9 wks and indicidual digits by about 12 weeks. The spine is recognized as two bright parallel lines at 7-8 weeks of gestation. |
|
|
|
|
|
8 weeks of
gestation |
|
|
|
|
|
|
|
|
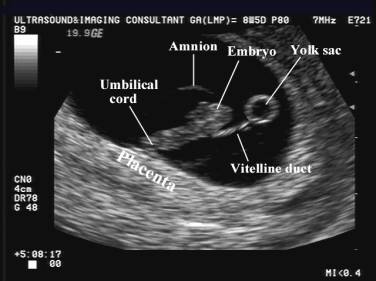
By 8 weeks of gestation the amniotic and chorionic cavities can be delineated as separate structures. The amniotic cavity progressively enlarges and fuses with the chorion at 12-16 weeks of gestation. |
|
Physiological bowel
herniation
|
|
|
|
|
|
Physiological herniation of the bowel occurs between 8.5 and 10.5 weeks and leads to elongation and rotation of the bowel. It is visualized as a swelling or mass in the base of the umbilical cord. By 12 weeks of gestation (when the crown rump length of the fetus reaches 45 mm) all the bowel should have returned to the fetal abdomen. |
|
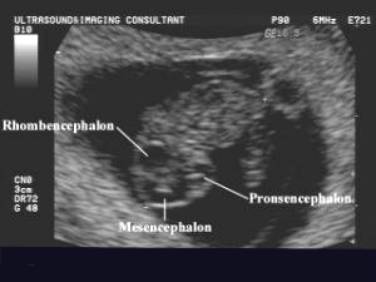
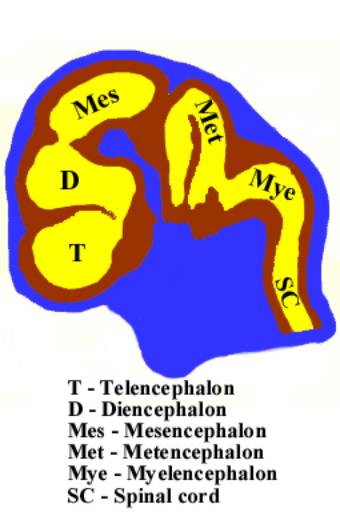
Week 9-12
|
|
|
|
|
|
The fetal brain vesicles are well delineated, however the chest and abdomen have few recognizable structures in the first trimester. The heart, stomach and physiological midgut herniation predominates. The “embryo” is termed a “fetus” at the end of the 10th menstrual week when organogenesis has ended. Thereafter growth and maturation of all tissue and organs occur. |
|