|
ANATOMY OVERVIEW –
SECOND AND THIRD TRIMESTERS |
Central Nervous System
|
||
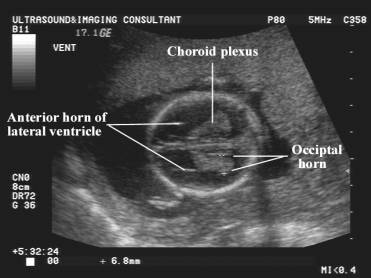
At 16 weeks the lateral ventricles consist of little more
than an anterior horn, body and small inferior horn. After 16 weeks there is
considerable growth of fetal brain structures. The lateral ventricles which
are a prominent feature of the brain in the early second trimester appears to
decrease in size relative to the cerebral hemispheres. The inferior and
occipital horns become elongated with progressive growth of the temporal and
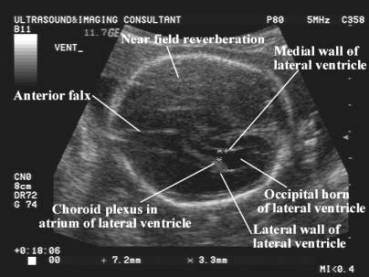
occipital lobes of the cerebrum. The highly reflective choroid plexus fills
the body of the lateral ventricle, however there may occasionally be some
fluid between the choroid plexus and medial or lateral ventricular wall. The
choroid plexus becomes progressively less prominent and is hard to discern in
the third trimester. Throughout the gestation the width of the lateral
ventricle rarely exceeds 9mm.
|
||
|
14
weeks of gestation |
|
|
|
28
weeks of gestation |
|
|
|
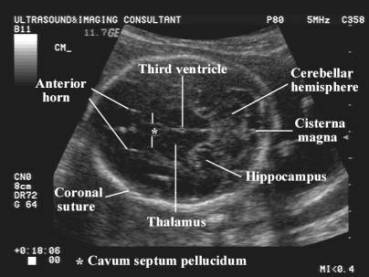
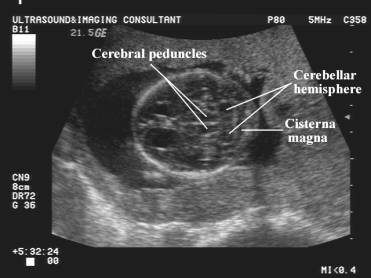
Most of the essential intracranial structures can be demonstrated on two axial views. The first view transects the lateral ventricles, the thalamic nuclei and third ventricle, the insula and Sylvian fissure (lateral cerebral sulcus) (see image of biparietal diameter). The second view is in a more caudal plane and transects the brainstem, cerebellum and cisterna magna. |
||
|
|
|
|
|
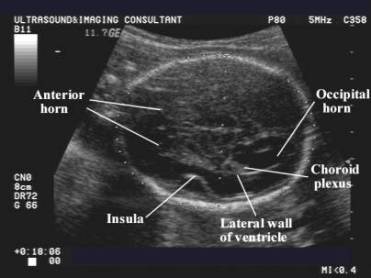
After the 20th week of gestation, the smooth surface of the brain becomes more convolute and the sulci and gyri start becoming evident. From about 22 weeks of gestation, the lateral sulcus between the medial insula and anterior migrating temporal operculum develop. This process is called opercularisation produces a linear echo lateral to but in the same scanning plane as the lateral ventricle. |
||
|
|
|
|
|
The medial walls of the lateral ventricle are formed anteriorly by the septum pellucidum, a double membrane that encloses a narrow cavity, the cavum septum pellucidum. This structure is visualized as a pair of parallel echoes close to the midline and just posterior to the echoes from the lateral walls of the anterior horn. It interrupts the midline anterior interhemispheric fissure about one-third of the distance from the frontal to occipital calvarium. |
||
|
|
|
|
|
The cerebellar hemispheres are bilateral symmetrical structures with a slightly more reflective rim. Their initial circular shape becomes progressively more triangular, and the central vermis, between the hemispheres, becomes more prominent with advancing gestation. The poorly reflective cerebral peduncles are anterior to the cerebellum, while the fluid filled cisterna magna is present posterior to the cerebellum and just in front of the occipital bone. |
||
Face
|
||
|
|
|
|
|
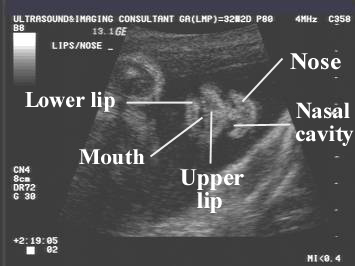
The Sagittal plane demonstrates the fetal profile and is good for assessing the relationship between the forehead, nasal bridge, lips and mandible. |
||
|
3D image of fetal face with a finger in the right eye. |
||
|
|
|
|
Chest + Heart
|
||
|
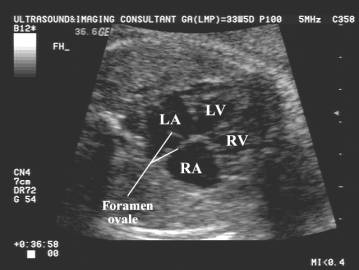
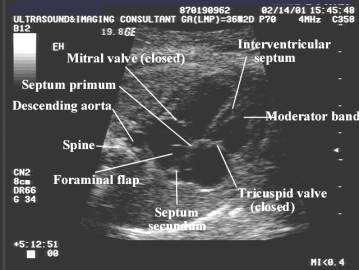
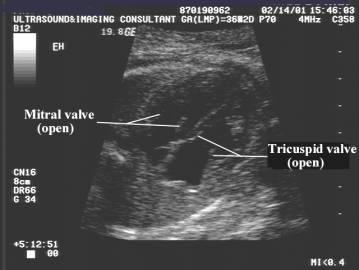
The cardiac chambers are assessed by the four-chamber view. The heart occupies about one-third of the chest cavity and is situated with the apex pointing towards the left side. The left atrium is the chamber that is most posterior (just anterior to the spine). The left ventricle lies posterolaterally and the right ventricle anteromedially. The foramen ovale and it’s flap are situated in the left atrium. The atrioventricular valves are evident separating the atria from their respective ventricles with the tricuspid valve situated slightly more inferior. The interventricular septum is a thick band of muscle separating the left from right ventricles. A band of tissue, the moderator band, is usually evident in the right ventricle. The aortic and pulmonary outflow tracts require special views to visualize. The myocardium and pericardium are usually inseparable unless a small amount of pericardial fluid is present. |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
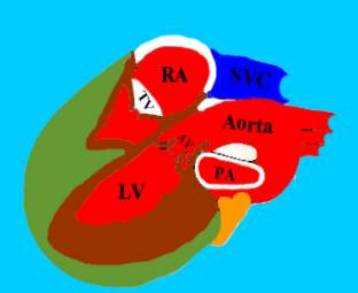
Aortic Outflow Tract – long and short axis views. |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
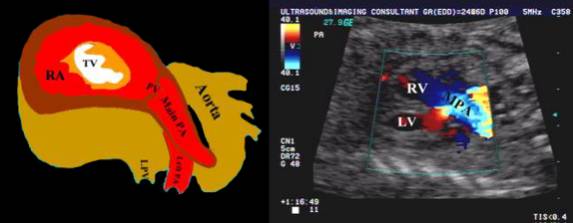
Ao – Aorta AV – Atrioventricular valve (mitral valve). DA – Descending aorta LA – Left atrium LPA – Left pulmonary artery LV – Left ventricle. MPA – Main pulmonary artery |
PA – Pulmonary artery PV – Pulmonary valve RA – Right atrium RPA – Right pulmonary artery RV – Right ventricle SVC – Superior vena cava TV – Tricuspid valve |
|
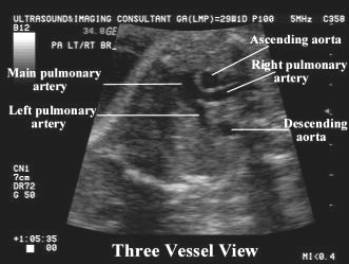
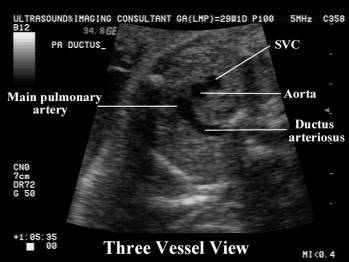
Pulmonary Outflow Tract |
||
|
|
||
|
|
||
|
|
|
|
|
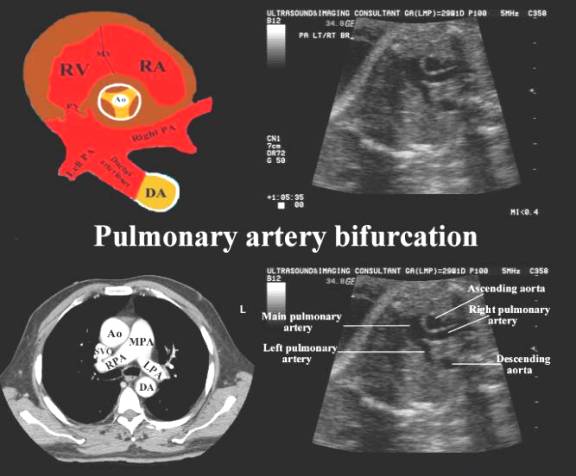
Major vessels in the superior mediastinum. |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spine
|
||
|
|
|
|
|
|
|
|
|
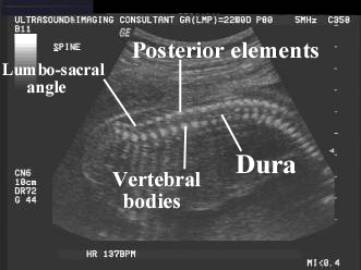
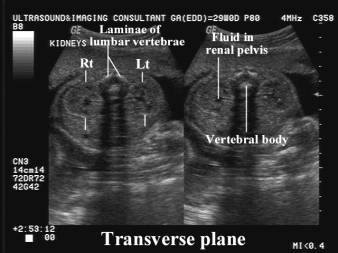
The vertebrae are formed from three ossification centers in fetal life; one for the vertebral body and one for each lamina of the neural arch. The spinous process only begins to ossify after birth. The ossification centers are seen as three reflective foci on a transverse (axial) image, surrounding the echo-free central neural canal. In the cervical, thoracic and upper lumber region they have a triangular shape, but become U-shaped in the lower lumbar spine due to the normal lumbar expansion of the neural canal. In the Sagittal view the anterior and posterior elements of the vertebral body are present as a double row of echoes (representing the vertebral bodies and laminae). |
||
|
|
|
|
Abdomen
|
||
|
The fetal liver occupies most of the upper abdominal cavity. The right lobe is larger than the left lobe and has a uniform low reflectivity. The umbilical vein enters the liver anteriorly and runs a 45 degree oblique course cephalad to join the posterior portal veins and enter the inferior vena cava via the ductus venosus. The gallbladder is an anechoic pear echo-free structure at the right inferior border of the liver (see images of Abdominal circumference). The spleen is situated posteriorly in the left upper quadrant of the abdomen. It has a uniform reflectivity, similar to liver. The fetal stomach should always be visualized as a fluid-filled structure by 14-16 weeks, however the small intestines and colon are not usually evident until the third trimester. |
||
|
|
|
|
|
|
|
|
Kidneys
|
||
|
|
|
|
|
|
|
|
|
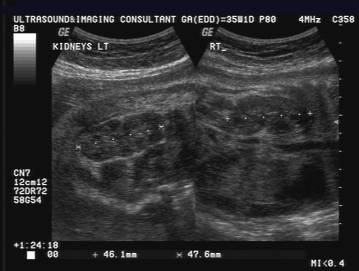
The kidneys are visualized on either side of the lumbar spine on transverse views. They have a homogeneous appearance and is constantly visualized from weeks 15-16 and onwards. The renal pelvis is an echo free space in he central portion of the kidney, with the medullary pyramids arranged as an echo-poor rosette around the pelvis. The renal capsule becomes visible at about 20 weeks as a dense thin reflective line. This line becomes brighter as perinephric fat is deposited with advancing gestation. The outline of the kidney becomes increasingly lobulated with advancing gestation (fetal lobulation). The ureters are not visualized unless they are obstructed. The urinary bladder should always be visualized as a round fluid-filled collection, while the urethra may only be evident during fetal micturition. The fetal adrenal glands are usually observed in a transverse or Sagittal plane just above the kidneys. They are usually evident by the 20th week of pregnancy and contain a dense echogenic central region (adrenal medulla) surrounded by a less dense peripheral portion (adrenal cortex). The adrenal glands are large in utero. |
||
Umbilical Cord
|
||
|
|
|
|
|
|
|
|
|
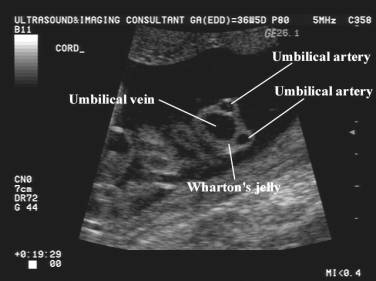
The umbilical cord contains a single umbilical vein and two umbilical arteries. In cross-section the appearance is that of “Mickey-mouse”. The larger vein transports oxygenated blood from the placenta to the fetus while the paired arteries transport deoxygenated blood from the fetus to the placenta. The cord usually inserts centrally into the placenta and into the fetus at the umbilicus. A collaginous material called Wharton’s jelly supports the spiralling umbilical arteries and umbilical vein. |
||
Placenta
|
||
|
|
|
|
|
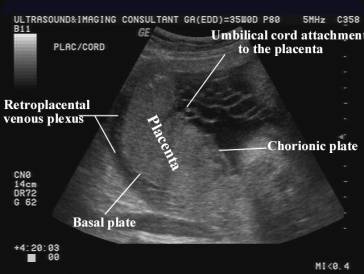
The placenta plays a major role in exchange of oxygen and nutrients between maternal and fetal circulations. The echo texture of the placenta is homogeneous and smooth and becomes more dense and calcified in the third trimester. It may implant in the uterine fundus, anterior or posterior uterine walls, laterally or occasionally over the cervix (placenta previa). The thickness of the placenta varies with gestational age from about 15mm to almost 50 mm at term. |
||
|
|
|
|