|
NORMAL FETAL KIDNEYS |
EMBRYOLOGY |
The kidney and its ureter develops in 3 stages. In each stage, which overlap each other to a small extent, a different set of excretory organs or kidneys exist. The 3 sets of kidneys develop in a cranial to caudal sequence
|
|
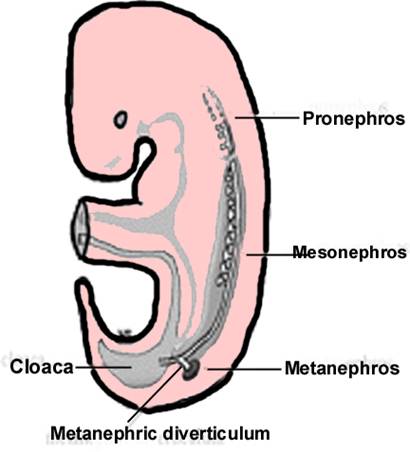
The first stage is termed the pronephros or forekidney after the nonfunctional pronephros that develops by the end of the third week of gestation and then regresses at 4 weeks. Tubules from the pronephros drain into the excretory duct that ends in the cloaca. (1-4).
The pronephros soon involutes, replaced by a somewhat more
caudal structure known as the mesonephros or midkidney, which incorporates most of the ducts of the pronephros. Cell clusters in the nephrogenic
cords develop lumina and become vesicles that grow
into urinefrous mesonephric
tubules each of which becomes associated with local blood vessels. The
combination of tubules and blood vessels develops into a glomerular
or Bowman’s capsule, the primitive glomeruli.
As the tubules from the lumbar region of the fetal
body develop, those in the thoracic area degenerate and disappear producing a
kidney in a low abdominal position. The tubules drain into an ipsilateral medial structure known as the Wolffian or mesonephric duct,
which drains into the excretory duct of the pronephros
stage.
The final stage of kidney development is that of the metanephros or hindkidney, the permanent kidney. It begins to develop in the latter portion of the fifth gestational week and begins functioning in the sixth week. It develops from mesodermal tissue at the most inferior aspect of the nephrogenic cord. At that site, metanephric blastema develops nephrons under the influence of the ureteric bud, a diverticulum of the mesonephric duct that develops at the level of the future first sacral vertebral body. Without a ureteric bud, no nephrons will develop. The ureteric bud on each side of the body elongates and divides multiple times and develop into the renal tubules, the calyces, the renal pelvis, and the ureters of that side of the body. The presence of individual calyces are necessary for the development of their associated primitive renal lobe made up of a renal pyramid and its surrounding renal cortex. By the 8th gestational week, the metanephros rises from its retroperitoneal position at the level of the sacrum to its normal position in which the renal hilum is at about the level of the second lumbar vertebral body.
Accessory renal arteries are common findings in life, because of persistence of the embryonic vessels, which fed the metanephros during its embryologic ascent (1-5). The metanephros becomes functional near the 12th week of gestation. By then, swallowed amniotic fluid is recycled through the kidneys and excreted as urine into the amniotic cavity that surrounds the fetus (4).
The metanephros arises caudal to the mesonephros at 5 weeks of development. It derives from mesoderm, the metanephrogenic blastema, lateral to the developing urogenital sinus and lateral to the mesonephric duct.
The ureteric bud arises as a diverticulum from the mesonephric (Wolfian) duct and invades the center of the metanephros. This juxtaposition of the ureteric bud and the specialized mesoderm stimulates the metanephrogenic blastema to form glomeruli, proximal and distal tubules. When the ureteric bud touches the metanephros, progressive branching of the ureteric bud occurs creating the renal pelvis, infundibulae, calyces, and collecting tubules which will provide a conduit for urine drainage in the mature kidney. This process is known as the induction of the kidney.
As the kidney develops in the elongating fetus, it 'ascends' from its original location (adjacent to the developing bladder) to its mature location (in the retroperitoneum just caudal to the diaphragm). As the kidney moves cephalad relative to the bladder, it takes new arterial supply from the aorta and new venous drainage into the vena cava. This "ascent" is also accompanied by medial rotation. Early in development, the renal pelvis lies anterior to the renal parenchyma. As the kidney moves into the lumbar region, the renal pelvis rotates medially so that the renal parenchyma lies lateral to the pelvis.
- Develop within the fetal pelvis in 7th menstrual week.
- Ascend into the posterolateral retroperitoneum by week 11.
- Nephrons form at about 10 weeks and urine production begins by weeks 13-15.
- Urine output increases from 2.2ml/hr at 22 weeks to 12.2ml/hr at 32 weeks and 28ml/hr at term.
ULTRASOUND |
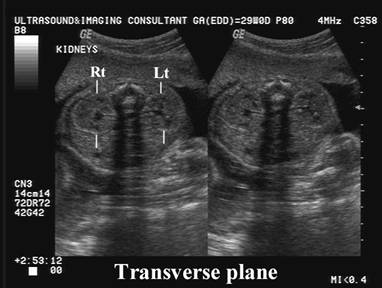
- Can be visualized early in the second trimester. Initially difficult to see, but increased perinephric fat improves sonographic contrast.
- Routinely seen by 16-18 weeks GA.
- Paired hypoechoic structures on either side of the fetal spine and shifts more laterally away from the spine as development progresses.

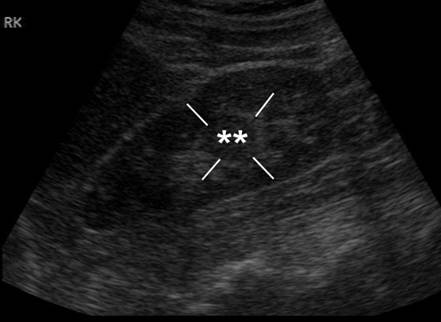
- Renal cortex is initially thin and difficult to visualize until the third trimester when the medullary pyramids and cortex can be visualized as separate entities. The medullae align along the pelvic sinus in a sagittal plane. Their relative hypoechoic appearance may be caused by the abundance of fluid-filled tubules.

- Renal sinus
- Central.
- Linear area of medium echogenicity.
- Visualized more frequently as the kidney grows and perinephric fat is deposited.
- Fetal lobulation (lobation is a better term as the renal lobule is a microscopic unit), as well as the medullary pyramids and collecting system can be well visualized in the third trimester.
|
|
|


- The typical fetal kidney is made up of discrete anterior and posterior lobes that fuse essentially 1 unit occurs by the 28th week of gestation. Irregularity to the border of some postnatal kidneys may be because of retained fetal lobulations. The medullary areas of individual renal lobes also tend to fuse preventing cortical tissue from extending in position. When the fusion is less than complete, cortical tissue may extend inferiorly and centrally and be adjacent to medullary tissue as a column of Bertin (1,2,7). Yeh et al (7) describe the hypertrophic column of Bertin as a normal variation because of unresorbed polar parenchyma of 2 subkidneys that fuse to form a normal kidney. Because the tissue is normal and not hypertrophic, they prefer the term "junctional parenchyma." An area of concern may be noted as junctional parenchyma rather than mass via US by noting that the area of concern contains renal cortex that is continuous and of similar echogenicity to that of the adjacent renal cortex (7).
|
Column
of Bertin |
|
|
|
|

Kidney length (Table) – Chervenak et.al. 1992
Kidney
volume (Graph) – Romero et.al. 1988
Kidney length (Table) – Chervenak et.al. 1992
Kidney volume (Graph) – Romero et.al. 1988
- Linear relationship of renal length to BPD.
- Renal length in mm = fetal menstrual age in weeks.
- Renal length (mm) = GA (wks) + 7.2 (95% CI ± 10).
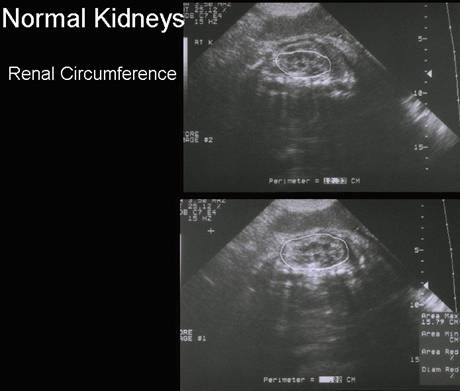
- Circumference.
- Renal area/abdominal area = 0.27 - 0.30 (constant from 24-38 wks).
|
|
{kind=link}
{kind=link}
- Transient fluid in the renal pelvis.
- Normal
renal length.
- Renal
Artery
REFERENCES |
- N.R.
Dunnick, C. Sandler,
E.S. Amis, Jr et al.. Textbook of Uroradiology
((ed 2).), Williams & Wilkins,
- K.L.
Moore and T.V.N. Persaud. The Developing
Human. Clinically Oriented Embryology (ed 7.),
Saunders,
- R.S. Narlawar, V. Hanchate, A. Raut et al., Renal agenesis and seminal vesicle cyst. J Ultrasound Med 22 (2003), pp. 225–228.
- T.W.
Sadler. Langman’s Medical Embryology (ed 9.), Lippincott Williams
& Wilkins,
- B. Cocheteux, C. Mounier-Vehier, V. Gaxotte et al., Rare variations in renal anatomy and blood supply: CT appearances and embryologic background. A pictorial essay. Eur Radiol 11 (2001), pp. 779–786.
- S.A.
Akbar, A. Shirkhboda
and H. Jafri,
- H.C. Yeh, K.P. Halton, R.S. Shapiro et al., Junctional parenchyma: Revised definition of hypertrophic column of Bertin. Radiology 185 (1992), pp. 725–732.