|
CLUBFOOT DEFORMITY
(TALIPES EQUINOVARUS) |
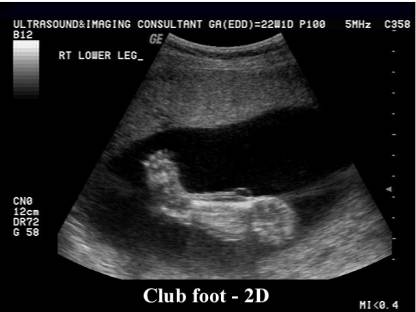
Clubfoot, or talipes equinovarus, is a deformity in which the foot is excessively plantar flexed, with the forefoot bent medially and the sole facing inward. This usually results in the underdevelopment of the soft tissues on the medial side of the foot and calf and to various degrees of rigidity of the foot and calf. The deformity is not passively correctable and does not resolve spontaneously.
· Incidence ranging from about 0.1% in the newborn population to 0.4% when diagnosed antenatally by ultrasound (1).
· The incidence of clubfoot varies with ethnicity:
· with a reported incidence of 0.4 per 1000 live births in Chinese,
· 1 to 5 per 1000 in whites,
· 6 to 8 per 1000 in Polynesians (2).
· Male fetuses are more commonly affected than females, with a 2:1 predisposition (3).
· Clubfoot is bilateral in approximately 50% of cases, but when unilateral is not predisposed to a particular side (4-6).
· Clubfoot can be isolated, or associated with other structural abnormalities. Other abnormalities are more likely to be present if clubfoot is diagnosed antenatally. For example, clubfoot has been associated with other structural abnormalities 10% to 14% of the time in neonatal series and as high as 80% in prenatal series (5,7,8).
· It can also be associated with many genetic syndromes (3,4).
Clubfoot is a combination of 4 deformities:
- Hindfoot equinus (reversed calcaneal pitch).
- Hindfoot varus (inward rotation; talocalcaneal angle of almost zero on AP view with bones parallel to each other).
- Forefoot adductus (axis of first metacarpal deviated medially relative to axis of talus).
- Variable forefoot cavus (plantar flexion).
|
21.5 weeks of gestation |
|
|
|
|
|
31 weeks of gestation |
|
|
|
|
|
|
|
|
|
|








CLASSIFICATION |
Clinical classification (9):
- Postural talipes – talipes that will correct with the normal growth of the child.
- Moderate talipes – talipes that requires conservative measures to correct, but may require surgical intervention.
- Severe talipes – talipes that does not respond to conservative measures and may be resistant to surgical intervention.
The feet are often classified retrospectively and no study has investigated the reliability of trying to classify them antenatally.
ETIOLOGY |
PATHOGENESIS |
ULTRASOUND |
- Diagnosis is based on demonstrating the tibia and fibula in the same plane as the lateral aspect of the foot, with the foot extended and inverted.
- Persistent (true clubfoot), transient (fetus can transiently turn foot into a position that simulates clubfoot) or relapsing (resolves in one scan and recurs in follow-up scans). Multiple images should be observed, preferentially with movement of the leg away from the wall of the uterus, to ensure that this is a fixed abnormality and not just a temporary positioning of a normal foot that mimics clubbing.
- Mild deformities may be more difficult to diagnose, because the foot may be turned inward but not entirely parallel to the lower leg
- Unilateral or bilateral.
- Classifies as postural, idiopathic or complex (other anomalies present which may not always be evident on antenatal scanning).
- Clubfoot can be diagnosed as early as 12 or 13 weeks, although it can be diagnosed in any trimester (1).
- The false-positive rate was reported in one series to be 11.8% (10).
- In one recently published retrospective series of 281 cases, the accuracy from 1987 to 1999 was only 35% (1). This improved to almost 70%, however, in the last year of that series. Accurate prenatal diagnosis is more likely when the condition is bilateral, or when there are associated abnormalities (1). In one study, all cases with associated anomalies were identified prenatally (11).
- The gestational age at which the etiology, rather than the diagnosis of the talipes, is confirmed is extremely important:
- Most complex cases (75%) are diagnosed at the 18-23 week scan (12).
- The remainder were diagnosed when the classification was changed from idiopathic to complex, either when scanned again after 24 weeks gestation (19%) or postnatally (6%).
- In this study 68 of the cases of talipes thought to be idiopathic at the 18-23 week scan, 13(19%) were subsequently found to be complex. This is important for counseling parents.
- Scan at 16-18 weeks does not exclude the diagnosis as late onset of clubfoot does occur.
- Jeanty and co-workers (14) describe two criteria for the diagnosis:
- Anteversion of the foot.
- Metatarsal rays are seen in the same plane, a medial to lateral plane that passes through the tibia and fibula and is perpendicular to the tibia and fibula.
|
|
|
|
|
|


- Rounded angle between the foot and lower leg (this sign may, however, be seen transiently in normal fetuses and is thus not pathognomonic).
- Tibia/fibula and foot (including toes) can be demonstrated simultaneously in their long axis i.e. foot deviates medially and lies at right angles to the tibia and fibula.
- Foot visualized in a plane perpendicular to the lower leg and not perpendicular to it.
- Foot must not be in an inverted position due to the confines of the uterus and is best diagnosed when the foot is completely surrounded by amniotic fluid.
- This position must be maintained for 10-30 minutes, as clubfoot may be transient. Follow up scans should probably be obtained in all cases. This excludes the false positive diagnosis of clubfoot.
Unilateral isolated clubfoot |
|
|
|
|
|
|
|
|
|
|





|
|
|
|
|
|
|
|

Sonographic detection of clubfoot warrants a detailed anatomic survey to search for any associated abnormalities. A fetal echocardiogram should be considered, and in the setting of associated structural abnormalities an amniocentesis should be recommended. There should also be a careful evaluation of the uterus looking for any evidence of uterine abnormalities, such as fibroids or a septum.
There is much controversy about whether to recommend amniocentesis after detection of an isolated clubfoot. It seems that clubfoot is associated with aneuploidy, but there are limited data adequately to quantify that risk. The data available are from small series of high-risk, selected populations (populations that were likely to need amniocentesis anyway), as opposed to low-risk populations in which these data are the most useful. Similarly, there are no data on the sensitivity, specificity, and positive or negative predictive value of clubfoot for predicting aneuploidy.
· Most studies have found that fetuses with clubfoot and karyotypic abnormalities usually have additional structural abnormalities (6).
· In one retrospective series of 35 cases of clubfoot, all five fetuses that had karyotypic abnormalities (four with trisomy 18, one with a translocation) had associated structural abnormalities (8).
· This is supported by the findings in another series of 51 fetuses with isolated clubfoot, in which there were no cases of fetal aneuploid (6).
· Other studies have suggested that clubfoot, even in the absence of associated abnormalities, confers increased risk of aneuploidy.
· In a recently published series of 87 fetuses identified as having isolated clubfoot, 4 fetuses (4.6%) had karyotypic abnormalities (one each of trisomy 18, trisomy 21, 47 XXY, and 47 XXX) (10). At least three of these women were considered high-risk for aneuploidy, however, and amniocentesis would have been recommended anyway: the two women with the sex chromosome abnormalities were over age 40, and the fetus with trisomy 18 had a single umbilical artery and clenched hands (diagnosed postnatally). The ultrasounds performed on the fetuses with the autosomal trisomies were performed at 15 and 16 weeks, and the early gestational age may account for the fact that the fetus with trisomy 18 had an undetected two-vessel cord and clenched hands. There is no mention in the results of whether multiple marker screens were performed on these fetuses and recent data indicate that integrated first- and second-trimester multiple marker screens can detect 80% to 90% of fetuses with trisomy 21 (13). Because from these limited data the predictive value of clubfoot for aneuploidy is unknown, and amniocentesis is associated with a risk of unintended loss, many clinicians do not recommend amniocentesis when the finding of clubfoot is isolated.
An argument against this approach is the concern for the possibility of missing associated abnormalities on ultrasound. In one series three (43%) of seven fetuses thought to have isolated clubfoot were diagnosed with additional anomalies after birth (8). None of these fetuses had karyotypic abnormalities.
ASSOCIATED ANOMALIES |
- Diastrophic
dysplasia.
- Osteogenesis imperfecta.
- Kniest dysplasia.
- Spondyloepiphyseal dysplasia
congenita.
- Metatrophic dysplasia.
- Mesomelic dysplasia (Nievergelt type).
- Chondrodysplasia punctata.
- Larsen
syndrome.
- TAR
syndrome.
- Pena-Shokeir syndrome.
- Roberts syndrome.
- Arthrogryposis multiplex congenita.
- Campomelic dysplasia.
- Myelomeningocele.
- Atelosteogenesis.
- Smith-Lemli-Opitz syndrome.
- Moebius sequence.
- Zelweger syndrome.
REFERENCES |
- . Keret D, Ezra E, Lokiec F, Hayek S, Segev E, Wientroub S. Efficacy of prenatal ultrasonography in confirmed club foot. J Bone Joint Surg Br 2002;84:1015-9.
- Dietz F. The genetics of idiopathic clubfoot. Clin Orthop 2002;401:39-48.
- Jones KL. Genetics, genetic counselling, and prevention. In: JonesKL,
editors. Smith's recognizable patterns of human malformation
-
-
- Malone FD, Marino T, Bianchi DW, Johnston K, D'Alton ME. Isolated clubfoot diagnosed prenatally: is karyotyping indicated? Obstet Gynecol 2000;95:437-40.
- Yamamoto H. A clinical, genetic and epidemiologic study of congenital clubfoot. Jpn J Hum Genet 1979;24:37-44.
- Rijhsinghani A, Yankowitz A, Kanis B, Mueller GM, Yankowitz KD, Williamson RA. Antenatal sonographic diagnosis of club foot with particular attention to the implications and outcomes of isolated club foot. Ultrasound Obstet Gynecol 1998;11:103-106.
- Maffulli N. Opinion: Prenatal ultrasonographic diagnosis of talipes equinovarus: does it give the full picture? Ultrasound Obstet Gynecol 2002;20:217-218.
- Shipp TD, Benacerraf
- Treadwell MC, Stanitski CL, King M. Prenatal sonographic diagnosis of clubfoot: implications for patient counseling. J Pediatr Orthop 1999;19:8-10.
- Bakalis S, Sairam S, Homfray T et.al. Outcome of antenatally diagnosed talipes equinovarus in an unselected obstetric population. Ultrasound Obstet Gynecol 2002;20:226-229
- Jeanty P, Romero R, d'Alton M et.al. In utero sonographic detection of hand and foot deformities. J Ultrasound Med 1985;4(11):595-601.