|
VELAMENTOUS CORD
INSERTION |
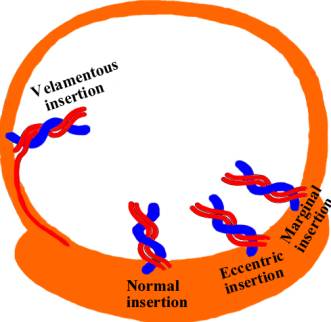
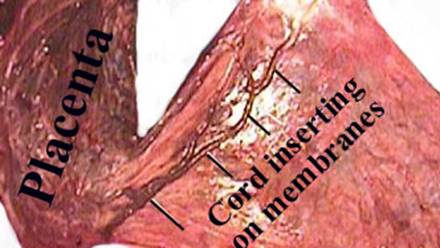
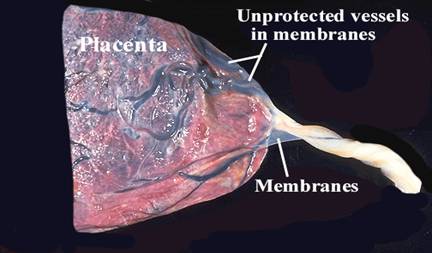
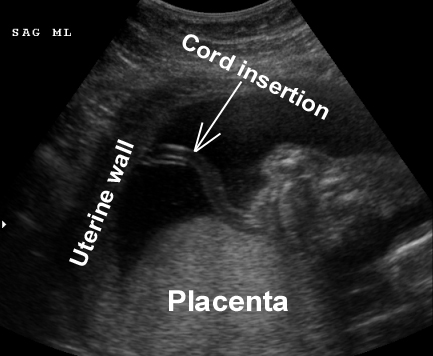
Umbilical cord inserting into the membranes of the placenta rather than onto the placental mass (1-11). The vessels are unsupported by either the umbilical cord or placental tissue. The vessels traverse the fetal membranes between the amnion and chorion prior to inserting into the placenta. The umbilical vessels separate from each other and course between the amnion and chorion before reaching the placenta.
INCIDENCE |
Common (1.1% of singleton births and 8.7% to 16% of twins deliveries) (1). In cases of monochorionic twin placentation, the frequency increases when the placentas are fused. The incidence of velamentous insertion is higher in early pregnancy: 33% between 9th and 12th weeks and 26% between 13th and 16th weeks (11).
PATHOGENESIS |
Several theories have been proposed including (1,11):
1. Abnormal fixation of the yolk sac to the chorion at a site which is distant from the definitive placental site.
2. Insertion of the body stalk to a region of proliferating trophoblast other than the decidua basalis (this theory propose that the umbilical cord arises from the chorion which is very vascular).
3. Abnormal primary implantation due to obliquity of the embryo during implantation.
4. Trophotropism (umbilical cord implants normally but becomes abnormal due to central atrophy and unidirectional lateral growth of the chorion frondosum).
|
|
|
|
Marginal cord insertion |
|
|
|
|
|
Velamentous cord insertion |
|
|
|
|
|
|
|
|
|
|

COMPLICATIONS (1-4) |
- Fetal exsanguination due to rupture vasa previa (mortality > 50%) (1,2). Vasa previa occurs when the vessels traverse the fetal membranes below the presenting part.
- Intrapartum hemorrhage.
- Fetal bradycardia.
- Twin-to-twin transfusion syndrome.
- Small for gestational age infants with a velamentous insertion of the cord is estimated to be 7,5% (5). In twin pregnancies, the twin with the velamentous cord insertion has a lower mean birth weight than the unaffected co-twin (5).
ASSOCIATIONS |
- IUGR (7.5%) (5-7).
- Congenital fetal anomalies (5.9% - 8.5%) (5,8) (esophageal atresia; obstructive uropathies, congenital hip dislocation; asymmetrical head shape; spina bifida; ventricular septal defects; single umbilical artery; bilobed placenta; trisomy 21).
- Preterm delivery (up to 17.2%) (5,9).
- Vasa Previa (1,2).
- Low birth weight, small for gestational age fetus (7).
- Single umbilical artery (10).
MANAGEMENT (8) |
- Careful scan to rule out fetal malformations.
- Follow up scans to exclude IUGR.
- Caesarean section prior to onset of labor or cervical dilatation.
REFERENCES |
- Benirschke K, Kaufmann P.
Umbilical cord and major fetal vessels. In: Benirschke K, Kaufmann P
(Eds): Pathology of the human placenta. 2nd Ed.
- Quek SP, Tan KL. Vasa Previa. Aust NZJ Obstet Gynecol 1972;12:206.
- Kouyoumdjian A. Velamentous insertion of the umbilical cord. Obstet Gynecol 1989;56:737-742.
- Paavonen J, Jouttunpaa K, Kangaslucoma P et.al. Velamentous insertion of the umbilical cord and vasa previa. Int J Gynaecol Obstet 1984;22:207-211.
- Bjoro K Jr. Vascular anomalies of the umbilical cord. I. Obstetrical implications. Early Hum Dev 1983;8:119.
- Scott JM, Jordan JM. Placental insufficiency and small for dates baby. Am J Obstet Gynecol 1972;113:823.
- Rolschau J. The relationship between some disorders of the umbilical cord and intrauterine growth retardation. Acta Obstet Gynecol Scand 1978;72(Suppl):15.
- Robinson LK, Jones KL, Benirschke K. The nature of structural defects associated with velamentous and marginal insertion of the umbilical cord. Am J Obstet Gynecol 1983;146:191.
- Brody S, Frenkel DA. Marginal insertion of the cord and premature labor. Am J Obstet Gynecol 1953;65:1305.
- Pretorius DH, Chau C, Poelyler DM et.al. Placental cord insertion visualization with prenatal ultrasonography. J Ultrasound Med 1996;15:585-593.
- Monie IW. Velamentous insertion of the cord in early pregnancy. Am J Obstet Gynecol 1965;93:276-281.