|
ABNORMALITIES OF THE
EARS |
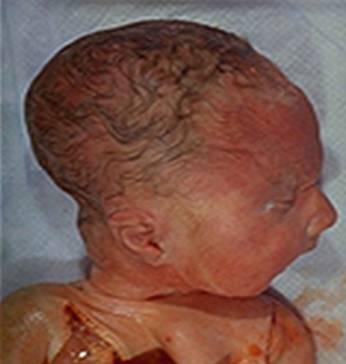
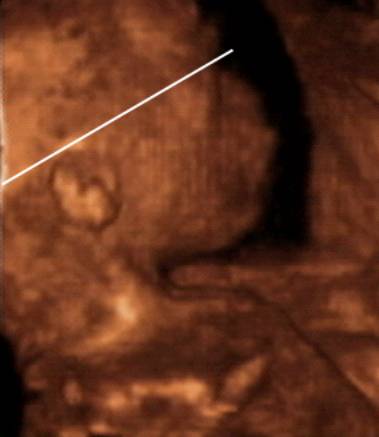
ANOTIA |
- Anotia is complete absence of the pinna of the ear.
- The skin of the cheek passes smoothly over the aural region without elevation or depression.
- The external auditory meatus is obliterated and the middle ear ossicles may be abnormal (1).
- Anotia is caused by deficient formation of the hillocks that produce the pinna and may be associated with facial paralysis, or a poorly developed tonsil on that side.
- There may be major malformations of the face and head.
- Bilateral anotia has been reported in children of consangineous parents (2).
- Anotia has been associated with thalidomide and retinoic acid embryopathy (3).
|
|
Anotia with cleft lip and palate. ·
Normal chromosomes. ·
No syndrome could be determined in this
fetus. |

REFERENCES |
- Ruzic J. Der sebiente fall kompletter anotia. Acta Otolaryngol 1948;36:186.
- Ellwood LC, Winter ST, Dar H. Familial microtia and meatal atresia in two sibships. J Med Genet 1968;5:289.
- Livingstone G. Congenital ear abnormalities due to thalidomide. Proc R Soc Med 1965;58:493.
SMALL EARS (MICROTIA) |
(>1.5 SD below gestational age average)
- Microtia is used to describe small pinnae, which is usually associated with other associated malformations such as cup shaped or overfolded pinnae (1).
- ± Abnormalities of the external auditory meatus (2).
- Non syndromic microtia has an autosomal dominant for of inheritance in a minority of patients. Isolated microtia is uncommon.
- Abnormally small ears have been noted to be one of the most consistent clinical findings in newborns and infants with trisomy 21 and other aneuploidies (5). Ears in these infants are usually described as small, low-set, malformed and posteriorly rotated.
- Ear anomalies have been described as a feature in as many as 60% of newborns with trisomy 21, as well as in more than 80-90% of those with trisomy 18 or trisomy 13 (6).
- Small ears does not appear to be a feature noted in association with sex chromosomal abnormalities. Turner syndrome is more often associated with prominent ears, and in infants with trisomy 4p syndrome, the ears are frequently enlarged with an abnormal helix and antihelix (6)
- Aase et al. (5) found that aside from hypotonia, short EL was the most consistent clinical characteristic in making the clinical diagnosis of Down syndrome. They also determined that in general, an ear length of 3.4 cm or less is usual for term newborn infants with Down syndrome. Although low-set position or posterior rotation of fetal ears is difficult to determine on ultrasound, measurement of fetal ears by ultrasound has been accomplished and reported in a few studies (6-10).
|
1. Trisomy 21. 6. Saethre-Chotzen syndrome. |
· Hemifacial macrosomia –
unilateral microtia, and failure of formation of the mandibular ramus and condyle.
Trisomy 13
·
Microtia. ·
Anophthalmos. |
|
|
|
|
|
Trisomy
18 ·
Small ears ·
Low set ears ·
Mild retrognathia |
|
|
|
|
|
|
|






LOW SET EARS (MELOTIA) |
- Defined as being present when the helix is attached to the cranium at a level below that of a horizontal plane with the corner of the orbit (4). Sonographically this definition is of limited value as a horizontal plane may be impossible to define.
- Ears are low when the attachment of the helix lies below the plane of a line joining the lateral angle of the orbit and inion.
- Most low set ears have a poorly formed cartilaginous skeleton to the pinna and may be folded over.
|
|
|
|
|
|
|
|
|




MACROTIA (LARGE EARS) |
- Large ears.
- Auricle is large but well shaped without other ear malformations.
- The scaphoid fossa is the most exaggerated portion of the ear.
- Usually bilateral and symmetric.
- Autosomal dominant inheritance in some cases.
- Associated anomalies:
- Marfan syndrome.
- Cerebro-oculo-facial-skeletal syndrome (COFS).
- Fragile X-syndrome.
- De Lange type 2 syndrome.
- Anophthalmia plus syndrome (bilateral Anophthalmia and an abnormal ear with absent lobule).

Fragile X
Syndrome
REFERENCES |
- Aase JM. Microtia - clinical observations. Birth Defects 1980;16:289.
- Livingstone G. Congenital meatal atresia. Proc R Soc Med 1964;57:1176.
- Livingstone G. Congenital ear abnormalities due to thalidomide. Proc R Soc Med 1965;58:493.
- Warkany
J. Congenital malformations: notes and comments.
- Aase JM,
 s
syndrome: a helpful diagnostic aid. J Pediatr
1973; 82: 845-7
s
syndrome: a helpful diagnostic aid. J Pediatr
1973; 82: 845-7 - Chromosomal syndromes: common and/or
well-known syndromes. In Gorlin RJ, Cohen MM,
Levin LS, eds. Syndromes of the Head and Neck , 3rd edn.
- Awwad JT, Azar GB,
- Chitkara U, Lee L, El-Sayed
Y, Holbrook RH. Bloch DA, Oehlert JW, Druzin ML. Sonographic ear length measurement in
normal second- and third-trimester fetuses. Am J Obstet
Gynecol 2000; 183: 230-4
- Shimizu T, Salvador L, Allanson J, Hughes-Benzie R, Nimrod C. Ultrasonographic measurement of fetal ear. Obstet Gynecol 1992; 80:
381-4
- Chitkara U, Lee L, Oehlert
JW et.al. Fetal ear measurements: a useful
predictor of aneuploidy? Ultrasound Obstet Gynecol
2002;19:131-134